INTRODUCTION
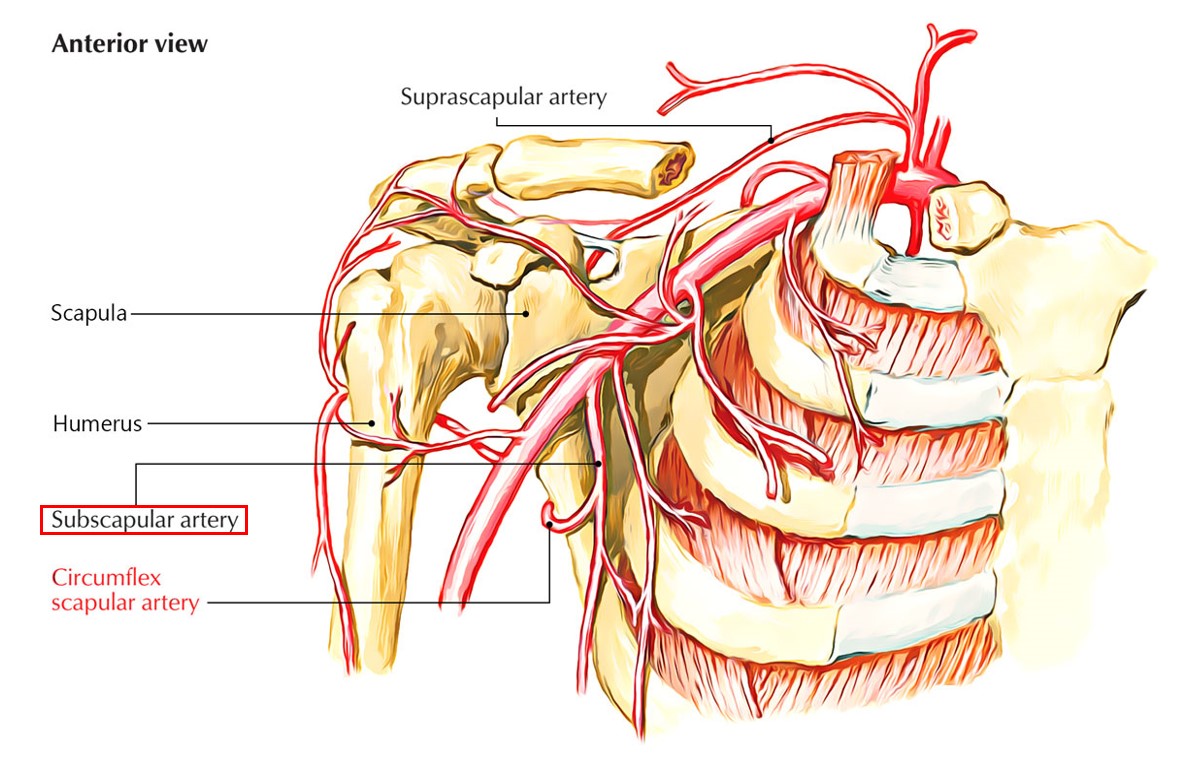
The axillary artery has a distal part. The largest branch of this part is known as the subscapular artery (SA) which proceeds inferiorly on the wall of the posterior axillary. It follows the subscapularis muscle exactly on the lateral margin. Two terminal branches are the end part of the subscapular artery (SA). These two terminals are the circumflex scapular and thoracodorsal arteries. The main function of these two terminal branches is to generate the anastomoses in the scapula region.
ORIGIN
In addition to serving as the largest branch, the subscapular artery is also the most variable part of the axillary artery. This branch usually arises from the third part of the axillary artery at the inferior border of the subscapularis muscle. Two clinical studies reported that the mean distance of the subscapular artery origin from the axillary artery was 7.3 cm and 6.69 cm, respectively.
BRANCHES
The subscapular artery (SA) consists of two large terminal branches including the thoracodorsal artery and circumflex scapular artery. The function of these two branches is as follows:
- The thoracodorsal artery proceeds anteroposteriorly along the scapula on its lateral border. On the way, this artery provides an increase to small branches that supply the two parts including adjacent skin and latissimus dorsi muscle.
- The larger part of the two terminal branches is known as the circumflex scapular artery. This branch proceeds posteriorly, encloses the lateral edge of the scapula, and arises on the posterior surface of the scapula. The circumflex scapular artery supplies the subscapularis muscles and teres major. This branch also gives collateral branches that take part in the formation of the anastomoses on the scapular artery.
SUPPLY
The subscapular artery is part of the axillary artery which has a large diameter and has two terminal branches. Due to these characteristics, the subscapular artery is responsible for supplying many of the muscles in the shoulder area. The muscles supplied by the subscapular artery are as follows:
- Supraspinatus muscle: This type of muscle is relatively small in size and upper back muscle that extends from the superior supraspinous fossa of the scapula to the greater tubercle of the humerus.
- Infraspinatus muscle: This muscle is relatively thick in size and structure as a triangular muscle. This muscle occupies the infraspinatus fossa in the main part This muscle is categorized as a rotator cuff muscle. It has the main function to stabilize the shoulder joint and externally rotate the humerus.
- Deltoid muscle: this muscle forms the rounded contour of the human shoulder.
- Latissimus dorsi muscle: this type of muscle is known as climbing muscle along your arms are still above your head, you can lift your torso, together with the help of the pectoralis major muscles.
- Serratus anterior muscle: this muscle is a fan-shaped muscle on the lateral wall of the thorax. Its main part is located deep under the scapula and pectoral muscles. It is easy to feel between the pectoralis major and latissimus dorsi muscles.
- Subscapularis muscle: this muscle is well defined as a large triangular muscle originating from the subscapular fossa. It is part of the four rotator cuff muscles, the other three being the supraspinatus, infraspinatus, and teres minor muscles.
- The long head of triceps brachii muscle: this muscle is a large muscle on the back of the upper limb of vertebrates. The medial head is mostly covered by the long and lateral head, and only visible distal to the humerus.
ANATOMICAL VARIANTS
The subscapular artery is part of the axillary artery which is quite stable from an anatomical point of view, with more than 80% showing its basic anatomy. Anatomical variations of the subscapular artery that may occur include:
- It arises from the second part of the axillary artery (about 15% of possibility)
- It is absent in just about 3% of circumflex scapular arteries and thoracodorsal artery which arise separately from the axillary artery.
- The lateral thoracic arteries, which possibly arise from the subscapular arteries
- The posterior humeral circumflex artery originates from the subscapular artery or the thoracodorsal artery.
- From the perspective of its origin, the subscapular artery could arise from the second or third part of the axillary artery. It is also could rise from the common trunk with a posterior circumflex humeral artery from an axillary artery, a common trunk with a lateral thoracic artery from the axillary artery, or a common trunk with a transverse cervical artery from the thyrocervical trunk of the subclavian artery.
Because the axillary artery including the subscapular artery has the highest rate of rupture rate and damage after the popliteal artery, knowing its variations is important and essential for anatomists, surgeons, and radiologists to decide the best clinical interventions for patients with an uncommon anatomical variant of the subscapular artery.
FUNCTION
The subscapular artery has the main function as a provider of blood supply to the shoulders, thoracic wall muscles, skin, and upper extremities. The muscles supplied by the subscapular artery have been mentioned above.
ABNORMALITIES
Some anatomical and physiological abnormalities case reports of the subscapular artery are as follows:
- Branching and bifurcation of the subscapular artery are found in a case study of 60 years old Greek male corpse. There are deep brachial arteries and superficial arteries in the 2nd section of the right-sided axillary artery. After generating the anterior humeral circumflex artery, the deep brachial artery is divided into branches and proceeds distally along the subscapular artery and the posterior humeral circumflex artery.
- A ruptured aneurysm disease is found on the left side of the subscapular artery of 74 years old woman with a medical history of type 1 neurofibromatosis. This ruptured aneurysm disease is clinically manifested with a sudden left chest mass and is later well diagnosed. This abnormality is caused by chronic occlusion of the left side subclavian artery. This circumstance is diagnosed with angiography before embolization. In conclusion, the collateral artery aneurysms in the presence of chronic occlusion of the major muscular arteries could develop in patients with a medical record of neurofibromatosis type 1.


 (82 votes, average: 1.73 out of 5)
(82 votes, average: 1.73 out of 5)