The hip joint is a ball-and-socket synovial joint where the femoral head acts as a ball and the socket is the acetabulum. This is considered as biggest ball and socket joint in the body. Due to its structure as a ball and socket, there is 360-degree encirclement is possible for the femur, also it rotates freely 90 degree on straight and side axis. However, it can perform one type of motion at a time while in motion.
The main functions of the hip joint are
- When standing, walking and running it supports the weight of whole body.
- Transfers and tolerates forces and pressures made by lower limbs (especially femur).
- It is multiaxial that allows a 360-degree encirclement and 90-degree side and straight axial motion.
- Provides structural stability to the Musculo-skeletal system.

Hip Joint
Type
The hip joint is a synovial joint of ball and socket assortment
Articular Surfaces
The head of the femur articulates with the horse shoe-shaped acetabulum of the hip bone to create the hip joint:
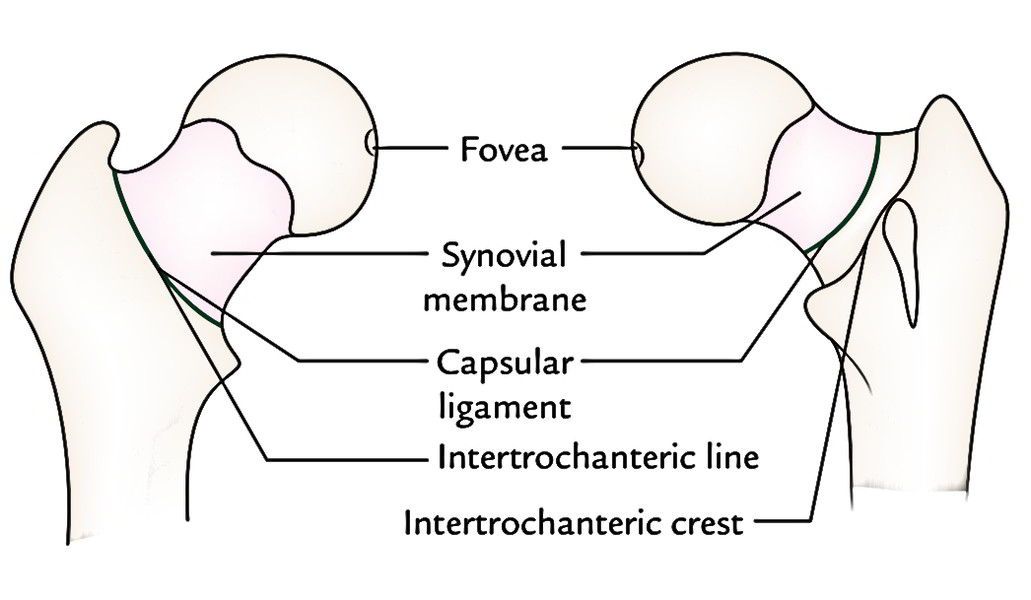
- The head of femur creates more than half of a sphere. It’s covered by the articular hyaline cartilage with the exception of a small pit- the fovea capitis for ligamentum teres.
- The acetabulum (Latin acetabulum = vinegar cup) presents 3 features: a horseshoe-shaped lunate surface, acetabular notch, and acetabular fossa. Out of these, only lunate surface is articular and covered by an articular cartilage. The depth of the acetabulum is raised by the acetabular labrum.
- Though proximal and distal articular surfaces are reciprocally arch but they’re not coextensive.
Ligaments
The ligaments of the hip joint are as follows:
- Capsular ligament (joint capsule).
- Iliofemoral ligament (most powerful).
- Pubofemoral ligament.
- Ischiofemoral ligament.
- Transverse acetabular ligament.
- Acetabular labrum.
- Ligamentum teres femoris (round ligament of the head of the femur).
Capsular Ligament
The capsular ligament is a powerful and dense fibrous sac which encloses the joint. Its attachments are as under:
- On the hip bone, it’s connected 5-6 millimeter past the acetabular margin, outer aspect of the acetabular labrum and transverse acetabular ligament.
- On the femur, it’s connected anteriorly to the intertrochanteric line and posteriorly 1 cm in front of (medial to) the intertrochanteric crest.
- The capsule is thicker anterosuperiorly, where the maximal stress takes place, especially in the standing position. Posteroinferiorly it’s thin and loosely connected.
- The capsule is made up 2 types of fibres- inner circular fibres and outer longitudinal fibres.
- The inner circular fibres create collar around the femoral neck (zona orbicularis). These fibres aren’t directly connected to the bones.
- The outer longitudinal fibres are represented along the neck toward the head to create the retinacula.
The synovial membrane lines inner aspect of the fibrous capsule, the intracapsular portion of the femoral neck, glenoid labrum (both surfaces), transverse acetabular ligament, ligamentum teres, and fat in the acetabular fossa. It’s thin on the deep surface of the iliofemoral ligament where it’s compressed against the head.
Iliofemoral Ligament
The iliofemoral ligament is an inverted Y-shaped ligament, which is located anteriorly and closely combined with the capsule. Its apex is connected to the lower half of the anterior inferior iliac spine and area between it and above acetabular margin. Its base is connected to the intertrochanteric line. This ligament includes 3 parts- a Lateral thick group of oblique fibres, a medial thick group of vertical fibres, and a large central thin portion.
Iliofemoral ligament is the most formidable ligament of body and prevents the trunk from falling backwards in the standing position.
Pubofemoral Ligament
The pubofemoral ligament is a triangular ligament with base above and apex below. It is located inferomedially and supports the joint on this particular aspect. Its base is connected to the iliopubic eminence, superior pubic ramus, and obturator crest. Inferiorly it combines with all the anteroinferior part of the capsule and medial group of the iliofemoral ligament.
Ischiofemoral Ligament
The ischiofemoral ligament is comparatively feeble and supports the capsule posteriorly. Above it’s connected to the ischium posteroinferior to the acetabulum. From ischium its fibresspiral behind the femoral neck to be connected into the greater trochanter deep to the iliofemoral ligament.

Hip Joint Ligaments
Round Ligament of The Head of Femur

Round Ligament of The Head of Femur
This ligament is also termed ligamentum teres of the head of femur. It’s a flat triangular ligament with apex connected to the fovea of the head, and its base to the transverse acetabular ligament. It’s ensheathed by a conical reflection of the synovial membrane. It will not raise the firmness of the joint.
- It conducts arteries to the head of the femur originated from the acetabular branches of the obturator and medial circumflex femoral arteries.
- Morphologically, the ligament of the head of femur composes the part of capsule that’s been comprised inside the joint.
Acetabular Labrum
The acetabular labrum is a fibro cartilaginous rim connected to the acetabular margin. It’s triangular in cross section. The labrum not only deepens the acetabulum (socket) but takes the head of femur softly to hold it in position.

Acetabular Labrum
Transverse Acetabular Ligament

Transverse Acetabular Ligament
It’s a part of acetabular labrum, which bridges the acetabular notch; nevertheless, it’s devoid of cartilage cells. The acetabular notch so becomes converted in the foramen which carries the acetabular vessels and nerves to the hip joint.
Stability of The Hip Joint
The firmness of the hip joint is supplied by the following factors which help prevent its dislocation:
- The depth of the acetabulum and narrowing of its mouth by the acetabular labrum.
- 3 powerful ligaments (iliofemoral, pubofemoral, and ischiofemoral) reinforcing the capsule of the joint.
- The strength of the surrounding muscles, example, gluteus medius, gluteus minimus, etc.
- Length and obliquity of the neck of femur.
Relationships
The Relations of the hip joint are as follows:
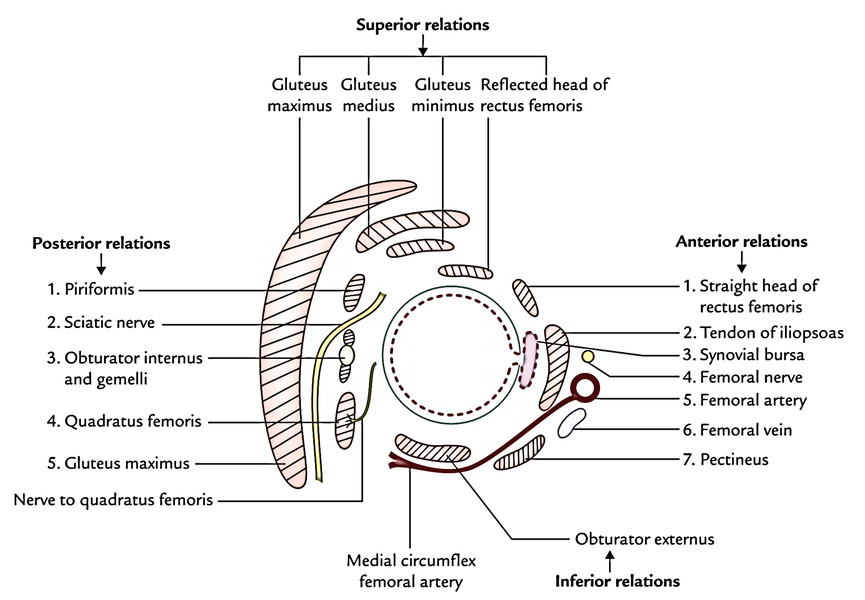
Anteriorly
- Tendon of iliopsoas divided from joint by a synovial bursa, pectineus (lateral part), straight head of rectus femoris.
- Femoral nerve in the groove between the iliacus and the psoas.
- Femoral artery in front of the psoas tendon.
- Femoral vein in front of the pectineus.
Posteriorly
- Piriformis, obturator externus, obturator internus, superior and inferior gemelli, quadratus femoris, and gluteus maximus.
- Superior gluteal nerve and vessels above the piriformis.
- Inferior gluteal nerve and vessels below the piriformis.
- Sciatic nerve, posterior cutaneous nerve of the thigh, and nerve to quadratus femoris.
Superiorly
- Reflected head of rectus femoris medially.
- Gluteus minimus, gluteus medius, and gluteus maximus laterally.
Inferiorly
- Pectineus.
- Obturator externus.
Bursae Around The Hip Joint

Bursae Around The Hip Joint
These are 7 in number: 4 under glutens maximus, 1 under gluteus medius, 1 under gluteus minimus, and 1 under psoas tendon as under:
- Between gluteus maximus and smooth area of the ilium being located between the posterior curved line and the outer lip of the iliac crest.
- Between gluteus maximus and lower part of the outer aspect of the higher trochanter (trochanteric bursa).
- Between gluteus maximus and ischial tuberosity (ischial bursa).
- Between the tendon of gluteus maximus and vastus lateralis (gluteofemoral bursa).
- 1 bursa below the cover of gluteus medius between it and upper part of the lateral aspect of the higher trochanter.
- 1 bursa below the gluteus minimus between it and anterior aspect of the higher trochanter.
- 1 between the iliopubic eminence and the psoas tendon. It’s termed subpsoas bursa. In 10% people the psoas bursa interacts together with the synovial cavity of the hip joint via a gap in the thin part of the capsule between the iliofemoral and pubofemoral ligaments.
Clinical Significance
Weaver’s backside: The subgluteal bursa between the gluteus maximus and ischial tuberosity is often inflamed and enlarged in individuals whose field demands long periods of sitting, example, weavers, leading to a clinical state referred to as weaver’s underside.
Arterial Supply
The hip joint is supplied by the branches of the following arteries:
- Medial circumflex femoral artery.
- Lateral circumflex femoral artery.
- Obturator artery.
- Superior gluteal artery.
- Inferior gluteal artery.

Arterial Supply of Hip Joint
The arterial supply of the head and neck of the femuris medically really essential. It’s originated from the following three sources:
- Acetabular branches of the obturator artery and the medial circumflex femoral arteries. These arteries get to the head via the round ligament of the head.
- Retinacular vessels (the main source) originate from the medial circumflex femoral artery, run along the neck of the femur via the retinaculum of the capsule.
- Nutrient artery of the femur supplies few branches to the neck and head of femur.
Nerve Supply
The hip joint is supplied by the following nerves:
- Femoral nerve via nerve to rectus femoris.
- A branch from anterior section of obturator nerve.
- A branch from accessory obturator nerve (if present).
- A branch from nerve to quadratus femoris.
- A branch from superior gluteal nerve.
- A twig from sciatic nerve (occasional).
4 straight spinal sections (L2, L3, L4, L5) control the movements of the hip joints as below:
- L2 and L3 modulate flexion, adduction, and medial rotation.
- L4 and L5 modulate extension, abduction, and lateral rotation.
Movements
The hip joint is a multiaxial joint and allows the following movements:
- Flexion and extension.
- Abduction and adduction.
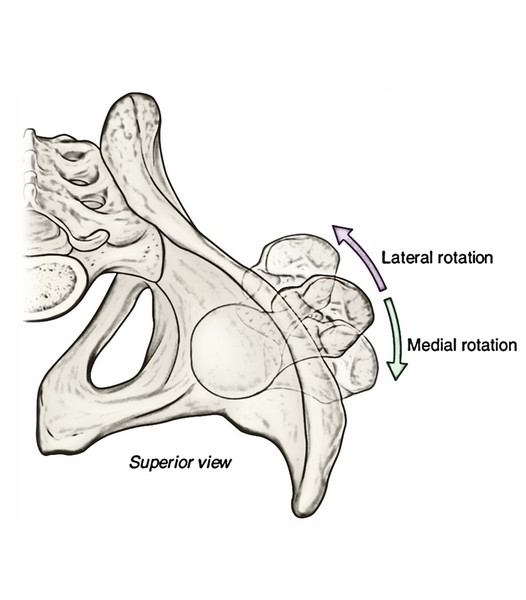
- Medial and lateral rotation.
- Circumduction (combo of the above movements).
The flexion and extension movements happen around the transverse axis, medial and lateral rotation take place around the vertical axis, and abductor and adduction movements take place around the anteroposterior axis.
Range of Movements
The flexion is 110 ° -120 °. It’s restricted by contact of the thigh with all the abdomen and adduction is restricted by contact together with the opposite thigh. The range of other movements is as below:
- Extension = 15 °
- Abduction =50 °
- Medial Rotation= 25 °
- Lateral Rotation= 60 °
Muscles Creating The Movements of The Hip Joint
| Movements | Muscles producing movements |
|---|---|
| Flexion | 1. Psoas major and iliacus (chief flexor) 2. Sartorius, rectus femoris, and pectineus |
| Extension | 1. Gluteus maximus (chief extensor) 2. Hamstring muscles |
| Abduction | 1. Gluteus medius and minimus (chief abductors) 2. Tensor fasciae latae and sartorius |
| Adduction | 1. Adductor longus, adductor brevis, and adductor magnus (chief adductors) 2. Pectineus and gracilis |
| Medial rotation | 1. Anterior fibres of gluteus minimus and medius (chief medial rotators) 2. Tensor fasciae latae |
| Lateral rotation | Piriformis, obturator externus, obturator internus and associated gemelli, quadratus femoris (These muscles are generally termed short rotators) |
Clinical Significance
Dislocation of The Hip Joint
(a) Congenital dislocation: The congenital dislocation of the hip joint is much more common than every other joint within the body. It happens because of two reasons:
- The joint capsule is loose at birth.
- Hypoplasia of the acetabulum and femoral head: In this state, the head of femur slips upward into the gluteal region since the upper margin of the acetabulum is developmentally deficient.
Medically, it presents as:
- Inability of the newborn to abduct the thigh.
- Affected limb is shorter in length and externally rotated.
- Asymmetry of skin folds of the thighs.
- Lurchinggait with positive Trendelenburg’s hint.
(b) Got dislocation: The acquired dislocation of the hip joint is unusual because this joint is extremely powerful and stable. Nonetheless, it might take place during a car accident when the hip joint is flexed, adducted, and medially rotated from the standard position of the lower limb when 1 is riding in an automobile. In this position, the joint is unstable as the femoral head is covered posteriorly by a joint capsule and not by the bone. During head on collision, the knee hits the dash and dislocates the hip joint. The head of the femur is forced out of the acetabulum by snapping the capsule posteroinferiorly and is located on the lateral surface of the ilium. This causes shortening and medial rotation of the affected limb.
The dislocation of the hip could be posterior (most common), anterior (less common), or central (least common). The sciatic nerve is injured in posterior dislocation.
Perthes’ Disease (Pseudocoxalgia)
It’s a clinical condition characterized by destruction and flattening of the head of femur with a greater joint space in the radiograph.
Coxa Vara And Coxa Valga
The normal neck-shaft angle is about 120 ° in adults and 160 ° in kids. If the neck shaft angle of the femur is reduced (example, fracture neck of femur, Perthes disease), it’s termed coxa vara. If the angle is raised (example, congenital dislocation of the hip joint), it’s referred to as coxa valga. This might come from Perthes disease, softening the neck because of rickets.
Osteoarthritis
It’s a disease of the old age. It’s defined by the development of osteophytes at the articular ends which not only restricts the movements but makes them grating and painful.
Referred Pain of The Hip Joint
In diseases of the hip joint like tuberculosis, the pain is referred to the knee joint due to the common Nerve Supply of these 2 joints.
Aspiration of The Knee Joint
It’s generally done by placing a needle 5 cm below the anterior superior iliac spine, upward, backward, and medially.
Fractures of The Neck of The Femur
Sadly, it’s sent as fractured hip meaning the hip bone is broken. These fractures are generally common in people of more than 60 years of age notably in females because their femoral necks become weak and fragile as a result of osteoporosis.
Types
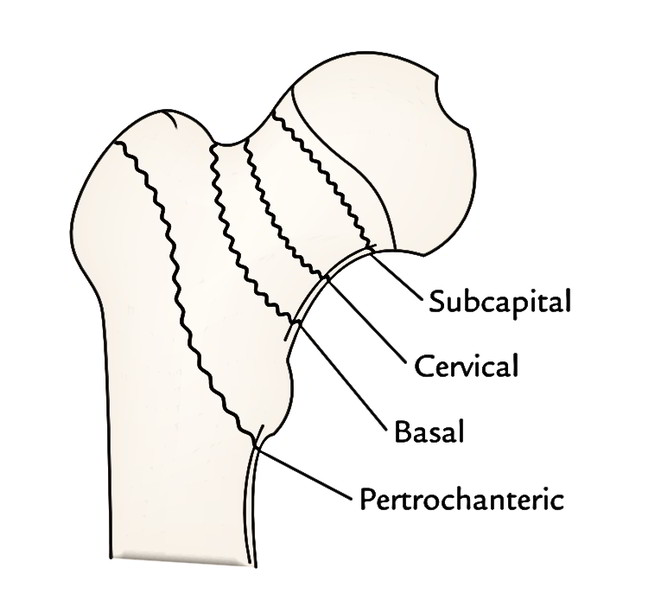
The fractures of the neck of femur are of 4 types:
- Subcapital (near the head).
- Cervical (in the middle).
- Basal (near the trochanters).
- Pretrochanteric fracture (just distal to 2 trochanters).
The retinacular vessels originated from the medial circumflex femoral artery supply majority of the blood to the head and neck of the femur. A pretrochanteric fracture (extracapsular fracture) doesn’t damage retinacular vessels, therefore avascular bone necrosis of head of femur doesn’t happen. Their damage in intracapsular fracture of the neck (i.e., subcapital and cervical) frequently result in aseptic bone necrosis of the head of the femur.
The fracture of the neck of the femur frequently takes place because of indirect violence of the insignificant nature. The individual falls down and can not get up. The affected limb is significantly shortened and rotated laterally. The diagnosis is usually supported by X-ray by discovering following 2 lines:
Shenton’s Line
In a radiograph of the hip region, the Shenton’s line is represented by a constant curved line created by the upper border of the obturator foramen and lower margin of the neck of the femur. This curve is interrupted in fractured neck of the femur or dislocation of the hip joint.
Schoemaker’s Line
It’s a straight line that goes from the tip of the higher trochanter to the anterior superior iliac spine and proceeds upward over the anterior abdominal wall to reach the umbilicus. If greater trochanter is elevated (example, fracture of the neck of femur) this line enters below the umbilicus.
Test Your Knowledge
Hip Joint

 (59 votes, average: 4.73 out of 5)
(59 votes, average: 4.73 out of 5)