The Knee Joint is the biggest and most complicated joint within the body. It holds and supports weight of the whole body. however, it is vulnerable to degradation with aging, that develops the condition of osteoarthritis, that is a disorder in which the joint cartilages and underlying bones start to break down and pain , stiffness, swelling and lower range of motion occur as primary symptoms. This is a widely studied topic due to its significance. The use of this joint in various physical activities and musculo-skeletal basis is highly significant.
Type
It’s a synovial joint of altered hinge variety. It’s not a normal hinge joint as it goes through some level of automatic (conjunct) rotation during flexion and extension of the knee.
Actually, it’s a compound joint being composed of 3 articulations: left and right condylar joints between the condyles of the femur and tibia, and 1 saddle joint between the femur and patella.
Articular Surfaces
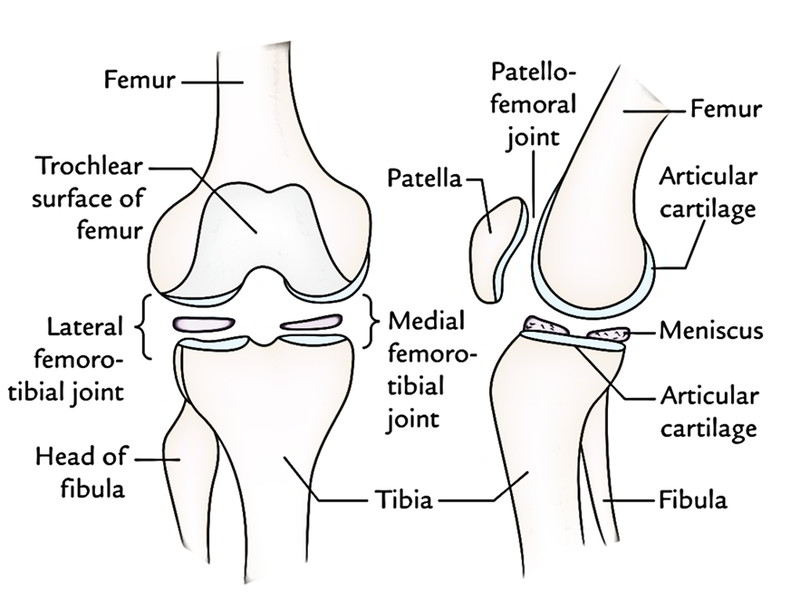
The articular surfaces of the knee joints are:
- Articular surfaces of medial and lateral condyles of the femur.
- Trochlear surface of the femur.
- Articular surface of the patella.
- Articular surfaces of medial and lateral condyles of the tibia.

The articular surfaces of the knee joints are described in detail in the subsequent text:
- Articular surfaces of medial and lateral condyles of the femur inhabit the anterior, inferior, and posterior surfaces of these condyles respectively. They can be convex anteroposteriorly and from side to side. The medial condylar surface is longer anteroposteriorly and narrower or mediolaterally than that of lateral condyle. Anteriorly they’re constant with every other via trochlear surface of the femur but posteriorly they’re divided from every other by an intercondylar notch.
- Trochlear surface of the femur can be found on the anterior aspect of the lower end of the femur. It articulates with all the posterior surface of the patella. It’s pulley-shaped, composed of medial and lateral sloping surfaces meeting with every other in a median vertical groove. The lateral sloping surface is longer than that of medial.
- Articular outermost layer of the patella is really on the posterior aspect of patella and articulates with the trochlear surface of the femur. It’s a bigger lateral area and a smaller medial area.
Near the medial margin of patella, there’s a narrow semilunar strip which comes in touch with a quite similar strip on the medial condyle of femur in total flexion. - Articular surfaces of the medial and lateral condyles of tibia are on the upper surfaces of these condyles. They’re divided from every other by a rough intercondylar area.
1. The articular surface on medial tibial condyle is oval and bigger. Its anteroposterior diameter is more compared to the transverse diameter.
2. The articular surface on the lateral tibial condyle is circular.
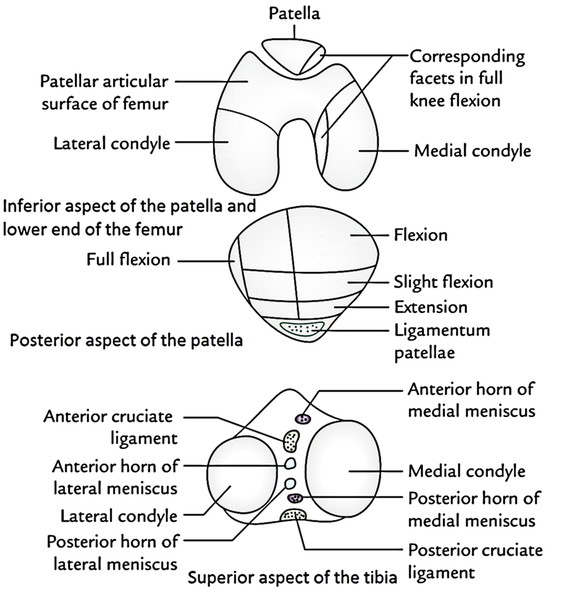
The articular surfaces on the upper surfaces of the medial and lateral condyles of the tibia are somewhat concave centrally and flat at the periphery where they’re covered by the corresponding menisci.
Stability of The Knee Joint
Structurally, the knee joint is comparatively poor mainly because of the incongruence of its articular surfaces. The tibial condyles are excessively small and shallow to hold the large convex femoral condyles. The femoropatellar articulation is also not quite stable due to their shallow articular surfaces and because of an outward angulation between the long axes of the femur and tibia.
Variables Keeping The Stability of The Knee Joint
The firmness of the knee joint is kept by these variables:
- Strength and Actions of the surrounding muscles and tendons.
- Medial and lateral collateral ligaments keep side-to side stability.
- Cruciate ligaments keep anteroposterior stability.
- Iliotibial tract helps in stabilizing a partially bent knee.
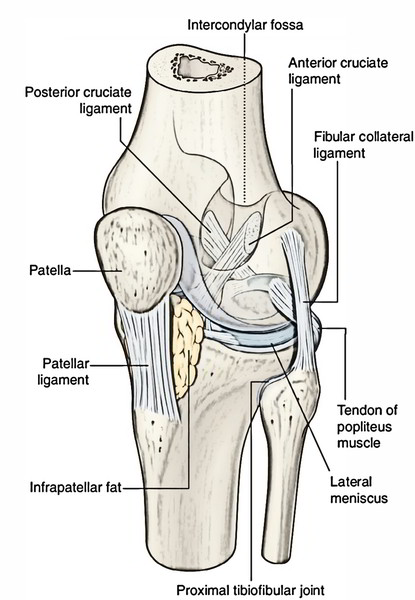
Ligaments
The significant ligaments of the knee joint are as follows:
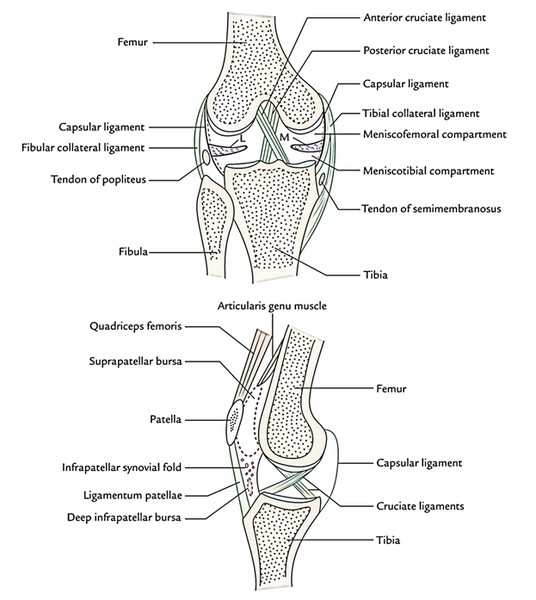
- Capsular ligament.
- Ligamentum patellae.
- Tibial and fibular collateral ligaments.
- Anterior and posterior cruciate ligaments.
- Medial and lateral menisci.
The other secondary ligaments of the knee joint are as follows:
- Oblique popliteal ligament.
- Arcuate popliteal ligament.
- Transverse ligament.
- Coronary ligaments.
All the ligaments are discussed in a separate article of Ligaments of knee Joint
Bursae Around The Knee
There are about 12 bursae around the knee, 4 anterior, 3 lateral, 3 medial, and 2 posterior.
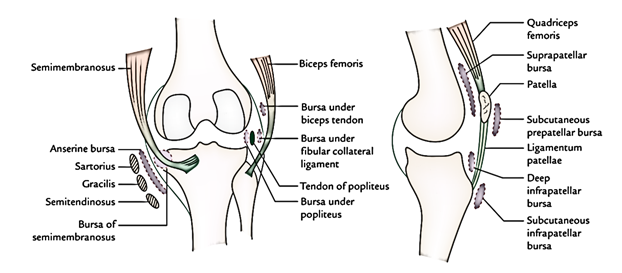
Anterior Bursae
These are:
- Subcutaneous prepatellar bursa (bursa of housemaid’s knee). It is located deep to the skin in front of lower half of the patella and upper half of the ligamentum patellae and tibial tuberosity.
- Subcutaneous infrapatellar bursa between the skin and smooth lower part of the tibial tuberosity.
- Deep infrapatellar bursa, between ligamentum patellae and tibial tuberosity.
- Suprapatellar bursa between the anterior surface of lower part of the femur and deep surface of the quadriceps femoris.
Lateral Bursae
These are:
- The bursa between the fibular collateral ligament and tendon of biceps femoris.
- The bursa between the fibular collateral ligament and tendon of popliteus.
- The bursa between the tendon of popliteus and lateral condyle of femur. This bursa is actually a synovial tube around the tendon of popliteus; thus it interacts with all the joint cavity.
Medial Bursae
These are:
- The bursa, which divides the tendons of sartorius, gracilis, and semitendinosus from every other and from the tibial collateral ligament (bursa anserine).
- The bursa between the tendon of semimembranosus and medial collateral ligament.
- The bursa between the tendon of semimembranosus and medial condyle of the tibia. It might convey together with the knee joint.
Posterior Bursae
These are:
- The bursa between the lateral head of gastrocnemius and capsule of the joint.
- The bursa between the medial head of gastrocnemius and capsule of the joint (Brodie’s bursa).
Clinical Significance
- Housemaid’s knee: It’s the inflammation of the prepatellar bursa (prepatellar bursitis). It takes place because of friction of bursa against the patella in regards in touch with all the earth during scrubbing of the floor by the housemaid. Such a bursa may get quite large and drop by its weight to much below to its first position.
- Clergyman’s knee: It’s the inflammation of subcutaneous infrapatellar bursa (subcutaneous infrapatellar bursitis). It takes place as a result of friction of bursa against the tibial tuberosity because of kneeling (example, kneeling during prayer by Christian priests/clergymen, roofers, and floor tilers.
- Baker’s cyst: The chronic inflammation of bursa deep to semimembranosus may present as cystic swelling in the medial part of the popliteal fossa termed Baker’s cyst.
Relations of The Knee Joint
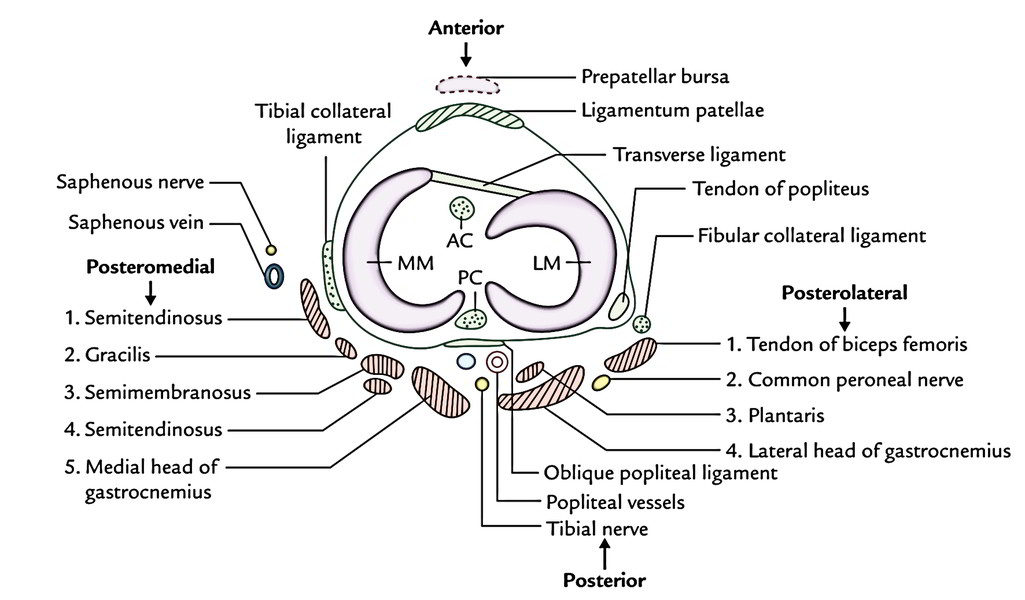
They’re as follows:
- Anteriorly: Tendon of the quadriceps femoris, patella, ligamentum patellae, patellar plexus of the nerves, and prepatellar synovial bursa.
- Anteromedially: Medial patellar retinaculum.
- Anterolaterally: Lateral patellar retinaculum and iliotibial tract.
- Posteriorly: Popliteal vessels, tibial nerve, and oblique popliteal ligament.
- Posterolaterally: In the upper part, tendon of biceps femoris and common peroneal nerve; in the lower part, lateral head of gastrocnemius and plantaris.
- Posteromedially: In the upper part, sartorius, gracilis, semimembranosus, and semitendinosus.
In the lower part, medial head of gastrocnemius and popliteus.
Blood Supply
The knee joint is lavishly furnished by the blood via the arterial anastomosis around the knee, that is created by:
(a) 5 genicular branches of popliteal artery, (b) descending genicular branch of femoral artery, (c) descending branch of the lateral circumflex femoral artery, (d) 2 recurrent branches of the anterior tibial artery, and (e) circumflex fibular branch of the posterior tibial artery.
Nerve Supply
The knee joint has abundant Nerve Supply by:
1. Femoral nerve via its branches to vasti, notably to vastus medialis.
2. Tibial and common peroneal nerves via their genicular branches.
3. Obturator nerve via its posterior section.
Movements
The following movements happen in the knee joints:
- Flexion.
- Extension.
- Medial rotation.
- Lateral rotation.
Flexion and Extension
These movements take place in the upper meniscofemoral compartment of the joint, i.e., above the menisci.
In flexion the angle between the posterior thigh and leg is decreased on the other hand in extension the angle between the posterior thigh and leg is raised (i.e., return from the flexion back to the anatomical position).
The movements of the flexion and extension at knee differ from average hinge movements in subsequent 2 manners:
- The transverse axis around which these movements happens isn’t repaired (example, during extension the axis moves forward and upward and during flexion it moves backward and downward).
- During these movements, there’s an automatic (conjunct) rotation of the knee (viz., medial rotation of the femur during last 30° of extension; and lateral rotation of the femur during first phases of the flexion). When foot is off the earth, tibia rotates rather than femur however in the opposite way.
Medial and Lateral Rotation
These movements take place in the lower meniscotibial compartment of the joint, i.e., below the menisci. These movements happen around the vertical axis.
The medial and lateral rotations normally happen with flexion and extension (conjunct turnings) but may take place alone if the knee is bent (adjunct turnings).
The conjunct turnings play an essential function in locking and unlocking of the knee.
Locking and unlocking of the knee:
- Locking of the knee: When the foot is really on the earth, the locking is defined as the medial rotation of femur on the tibia during the terminal stage of extension of the knee. When the knee is locked it becomes completely stiff and all the ligaments of the joint are tight. This is called “screw house mechanism”.
- Unlocking of the knee: When the foot is really on the earth, the unlocking is defined as the lateral rotation of the femur on the tibia during first stage of the flexion. The unlocking is brought about by the popliteus muscle. When the knee is unlocked, it can be farther contracted by the hamstring muscles.
The locking of knee is crucial for bearing load during erect pose. The fast joint must be unlocked to facilitate advance of locomotion. Therefore, during locomotion locking and unlocking of the knee occurs instead and rhythmically.
The differences between the locking and unlocking of the knee are as summarized in the box below:
Locking of the knee joint | Unlocking of the knee joint |
|---|---|
| • Medial rotation of the • Lateral rotation of the femur on tibia during femur on tibia during initial terminal phase of extension phase of the flexion | |
| • It is brought about by quadriceps femoris | • It is brought about by the popliteus muscle |
| • Locked knee becomes absolutely rigid | • Unlocked knee can be further flexed |
| • All ligaments are taut | • All ligaments are relaxed |
Movements of The Knee Joint
Muscles producing movements | ||
|---|---|---|
| Movements | Chief muscles | Accessory muscles |
| Flexion | Semimembranosus | Popliteus |
| Semitendinosus | (initiates flexion) | |
| Biceps femoris | 1.Sartorius. | |
| 2.Gracilis | ||
| 3.Gastrocnemius. | ||
| 4.Plantaris. | ||
| Extension | Quadriceps femoris | Tensor fasciae latae |
| Medial rotation | 1.Semitendinosus. | 1.Sartorius. |
| 2.Semimembranosus. | 2.Gracilis. | |
| 3.Popliteus. | ||
| Lateral rotation | Biceps femoris | 1.Gluteus maximus. |
| 2.Tensor fasciae latae | ||
The range of motion (ROM) of flexion is 130 °, on the other hand, the range of motion of expansion is 0-50°.
The ROM for flexion is greater when the hip joint is fixed. The ROM for extension is greater when the hip is extended and restricted when the hip is flexed.
Clinical Significance
Osteoarthritis
Being a weight bearing joint, the knee joint is often included in osteoarthritis (degenerative wear and tear of articular cartilages). The movements might be distressing, small, and create grating. Radiographs of the knee region show osteophytes, i.e., peripheral lipping of the articular ends.
Injuries To Cruciate Ligaments
The anterior cruciate ligament is more typically damaged in relation to the posterior ligament. The anterior cruciate ligament is injured in the anterior dislocation of the tibia; on the other hand, the posterior ligament is injured in the posterior dislocation of the tibia. Rip of the cruciate ligaments contributes to abnormal anteroposterior freedom.
If the anterior cruciate ligament is torn the tibia is pulled excessively forward on the femur (anterior drawer sign) and if the posterior cruciate ligament is torn the tibia is pulled excessively backwards (posterior drawer sign).
Aspiration of The Knee Joint
The collections of fluid are typical in the knee joint. It provides rise to swelling above and at the sides of the patella. In such cases, patellar tap regularly shows a floating patella. Aspiration of the fluid can be carried out on each side of the ligamentum patellae. Nevertheless, the joint is generally approached from its lateral side using 3 bony points as landmarks for the needle insertion:
(a) tibial tuberosity, (b) lateral epicondyle of the femur, and (c) apex of patella. This triangular area is also utilized for drug injection in treating the knee pathology.
Arthroscopy of The Knee Joint
It’s an endoscopic evaluation (visualization) of the inner part of the knee joint cavity with nominal disruption of the tissues. The ligament repair or replacement can also be performed by using an arthroscope.
Knee Replacement
If the knee joint is badly damaged by the osteoarthritis, an artificial joint being composed of plastic tibial component and alloy femoral component is linked to the tibial and femoral bone ends after removal of the damaged regions.
Miserable Triad of The Knee Joint
A combo of injury of the (a) tibial collateral ligament, (b) medial meniscus, and (c) anterior cruciate ligament is named” sad triad” of the knee joint.
Test Your Knowledge
Knee Joint

 (66 votes, average: 4.44 out of 5)
(66 votes, average: 4.44 out of 5)