The larynx is altered for generating voice and is the upper enlarged part of the lower respiratory tract, therefore it’s also named voice box/organ of phonation. It functions as a sphincter in the inlet of lower respiratory tract and to safeguard the trachea and the bronchial tree from entrance of any material besides the air. Laryngeal incompetence results and food and fluid could possibly be aspirated into trachea, if this protective function is deranged. Farther, the upward and downward movements of the larynx help in consuming.
Functions
- Phonation.
- Respiration.
- Protection.
- Deglutition.
The primary (most significant) function of the larynx is protection of the lower respiratory tract. The phonation has grown afterwards with development and is associated with the motor speech area of the brain.
Location and Extent
The larynx is situated in the anterior midline of the upper part of the neck before laryngopharynx. It goes from the root of the tongue to the trachea and is located in front of the 3rd, 4th, 5th and 6th cervical vertebrae. Nonetheless, in kids and females it is located at a little higher level.
Size
The typical measurements of larynx in males and females are as follows:
| Vertical | Transverse | Anteroposterior | |
|---|---|---|---|
| Male | 44 mm | 43 mm | 36 mm |
| Female | 36 mm | 41 mm | 26 mm |
Till puberty the size of larynx in both males and females is more or less same but at puberty male larynx grows quickly and becomes bigger in relation to the female larynx. The pubertal development of the larynx in adult female doesn’t differ much from a child, for this reason the pitch of voice is high in both females and youngsters. In men, the characteristic pubertal increase of angle of the thyroid cartilage (Adam’s apple) makes the voice louder and low pitched.
Skeleton
The skeletal framework of the larynx is made up of series of cartilages that are linked to 1 another by ligaments and fibrous membranes and proceeded by a number of muscles.
The hyoid bone is closely connected to the larynx with distinguishing functional purposes. Yet, it’s generally regarded as another structure.
Cartilages
The larynx consists of nine cartilages, of which 3 are unpaired and 3 are matched:
Unpaired cartilages: The unpaired cartilages are large and include:
- Thyroid.
- Cricoid.
- Epiglottis.
Matched cartilages: The matched cartilages are small and constitute:
- Arytenoid.
- Corniculate.
- Cuneiform.
The primary cartilages of the larynx are cricoid, thyroid and 2 arytenoids.
Joints
The laryngeal joints contain matched cricothyroid, cricoarytenoid and arytenocorniculate joints.
Cricothyroid Joint
It’s a plane synovial joint between the inferior cornu of the thyroid cartilage and side of cricoid cartilage. The recurrent laryngeal nerve enters the larynx quite close to this joint. This joint allows 2 types of movements, viz.
Rotatory movement when cricoid rotates on the inferior cornua of the thyroid cartilage around a transverse axis, which enters transversely via both cricothyroid joints.
Gliding movement, where cricoid glides, to a small extent, in distinct ways of the thyroid cornua.
Cricoarytenoid Joint
It’s a miniature plane synovial joint between the base of the arytenoid and lateral part of the upper border of the lamina of cricoid cartilage. This joint allows 2 types of movements, viz.
- Rotatory movement, where arytenoid cartilage moves around a vertical axis, so abducting or adducting the vocal cords.
- Gliding movement, where 1 arytenoid glides in the direction of the other or far from it, hence shutting or opening the posterior part of glottis.
Arytenocorniculate Joint
It’s a synovial joint between the arytenoid and corniculate cartilages. It’s of no functional value.
Ligaments and Membranes
The skeletal framework of the larynx is interconnected by a number of ligaments and fibrous membranes. The most crucial fibrous membranes linking skeletal framework of the larynx are thyrohyoid, cricothyroid, quadrangular and cricovocal membranes.
Extrinsic
The extrinsic ligaments and membranes are outside the inner tube of the fibroelastic tissue of laryngeal cavity.
Thyrohyoid membrane and ligaments: The thyrohyoid membrane stretches from the upper border of the thyroid cartilage to the upper border of the hyoid bone. It ascends behind the concave posterior surface of the hyoid bone. Between posterior aspect of hyoid and membrane is located the subhyoid bursa. In the median and lateral parts, the thyrohyoid membrane thickens to create median and lateral thyrohyoid ligaments. The lateral thyrohyoid ligament on every side includes a small nodule of elastic cartilage termed cartilago triticea. The thyrohyoid membrane is pierced on each side by internal laryngeal nerve and superior laryngeal vessels.
- Cricotracheal ligament: It attaches the cricoid cartilage with the first tracheal ring.
- Thyroepiglottic ligament: It attaches the lower narrow end of epiglottis to the posterior surface of thyroid angle.
- Hyoepiglottic ligament: It attaches the posterior aspect of hyoid with the anterior surface of the upper end of epiglottis.
- Cricothyroid ligament: It attaches the lower border of the thyroid cartilage to the cricoid cartilage in the midline.
Intrinsic
The intrinsic ligaments and membranes are the parts of a broad sheet of fibroelastic tissue, which creates the inner tube of the laryngeal cavity outside its mucous lining. This fibroelastic tube is, nevertheless, interrupted on every side by the sinus of the larynx. The part above the sinus is referred to as quadrate or quadrangular membrane and part below the sinus is named cricovocal membrane or conus elasticus:
Cricovocal membrane extends upwards and medially from the upper border of the arch of the cricoid cartilage. Its upper edge is free and connected anteriorly to the posterior surface of the thyroid cartilage and posteriorly to the vocal process of the arytenoid cartilage. It’s somewhat thickened to create the vocal ligament. The fold of mucous membrane over this ligament creates the vocal fold.
Vocal ligament is created from yellow elastic tissue and goes anteroposteriorly from posterior surface of the thyroid cartilage to the vocal process of arytenoids cartilage.
Quadrangular membrane goes from sides of epiglottis to the arytenoids. Its lower border is free and connected anteriorly to the posterior surface of the thyroid cartilage (above the cricothyroid membrane) and posteriorly tothe lateral surface of the arytenoid cartilage (in front of muscular process). Its lower border is thickened to create the vestibular ligament.
Vestibular ligament is created from fibrous tissue and goes anteroposteriorly from posterior surface of the thyroid cartilage to the lateral surface of the arytenoid cartilage.
Extrinsic and Intrinsic Membranes and Ligaments of The Larynx
| Extrinsic | Intrinsic |
|---|---|
| • Thyrohyoid | • Cricovocal (conus elasticus) |
| • Cricotracheal | •Quadrate/Quadrangular |
| • Median and lateral thyrohyoid | • Vocal |
| • Cricothyroid | • Vestibular |
| • Cricotracheal | |
Muscles
They’re of 2 types: extrinsic and intrinsic.
Extrinsic
They connect the larynx to the surrounding structures and are liable for the movement of the larynx as a whole.
All the extrinsic muscles are coupled and contain:
- Palatopharyngeus.
- Salpingopharyngeus.
- Stylopharyngeus.
- Thyrohyoid.
- Sternothyroid.
All these muscles elevate the larynx with the exception of sternothyroid, which depresses the larynx.
Intrinsic
They connect the laryngeal cartilages to every other and are liable for their movements. Their principal functions are to:
- Open or shut the laryngeal inlet,
- Adduct and abduct the vocal cords and
- Raise or reduce the tension of the vocal cords.
Therefore according to their intrinsic muscles of the larynx are ordered into these groups:
Muscles That Open or Shut the Laryngeal Inlet
- Oblique arytenoids.
- Aryepiglotticus.
- Thyroepiglotticus: opens the inlet of larynx.
Muscles That Abduct or Adduct Vocal Cords The
- Posterior cricoarytenoids: abduct the vocal cords.
- Sidelong cricoarytenoids: adduct the vocal cords.
- Transverse arytenoid: adduct the vocal cords.
Muscles That Increase or Decrease the Tension of Vocal Cords
- Cricothyroid: strains the vocal cords.
- Vocalis: strains the vocal cords.
- Thyroarytenoid: unwinds the vocal cords.
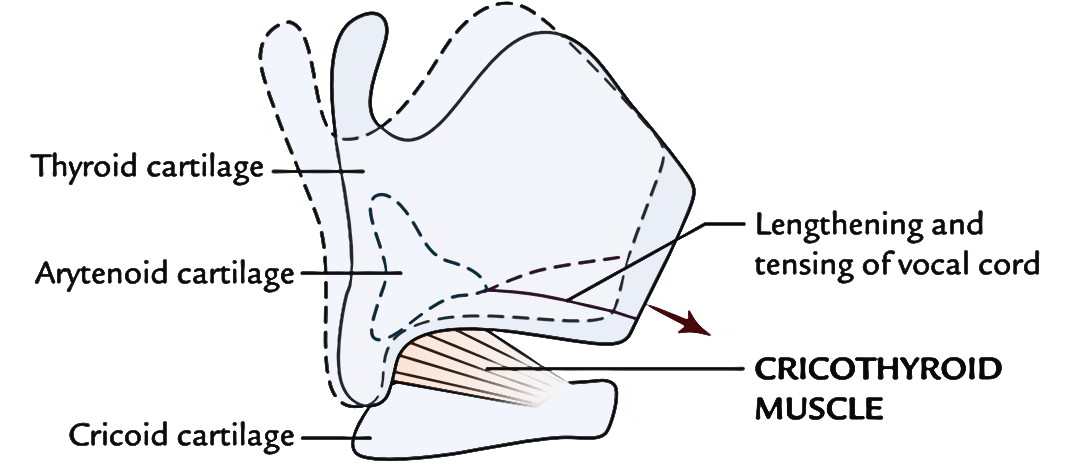
Cricothyroid Muscle
It’s the only muscle of the larynx, which is located on the external outermost layer of the larynx.
It’s a small fan-shaped muscle, which originates from the anterolateral aspect of the cricoid. After origin, its fibres pass backwards and upwards, to be added into the inferior cornu and adjacent lower border of the lamina of the thyroid cartilage. It’s supplied by external laryngeal nerve. Its contraction gets the thyroid cartilage to lean somewhat downwards and forwards at the cricothyroid joints, thus lengthening and straining the vocal cord. It also helps in adduction of vocal cord.
The entire thyroid cartilage can move downwards and forwards over the cricoid like the Visor of a knight’s helmet (Grant).
Clinical significance
The cricothyroid is a significant muscle for the tone and pitch of the voice. When sound is going to be created, it strains the vocal cord and makes it prepared to vibrate as a tuning fork. For this reason it’s also called the tuning fork of larynx. Paralysis of the muscle following external laryngeal nerve lesion changes the voice fairly substantially and is particularly noticeable in vocalists.
Vocalis Muscle
It’s the degage medial part of the thyroarytenoid and is located inside the vocal fold just lateral and cranial to the vocal ligament. It originates from the thyroid angle and anterior part of vocal ligament and fit into the lateral surface of the vocal process. On its contraction the anterior part of vocal ligament strains on the other hand its posterior part is rested.
It’s supplied by the recurrent laryngeal nerve.
The segmental tension of vocal ligament helps in the modulation of voice such as the fingers of a violinist.
Posterior Crico-arytenoid
It’s a triangular muscle, which originates from the posterior surface of the cricoid lamina lateral to its median ridge. After origin, the fibres pass upwards and laterally to be added into the rear of the muscular process of the arytenoid.
It’s supplied by recurrent laryngeal nerve.
The posterior cricoarytenoid abducts the vocal cords.
Clinical significance
Safety muscles of larynx: The posterior cricoarytenoid muscles are the only intrinsic muscles of the larynx, which abduct the vocal cords to enable entrance of air via rima glottidis in the respiratory tract below it.
When posterior cricoarytenoids contract, muscular processes of both the arytenoid cartilages rotate medially. Because of this, the vocal processes rotate laterally (abducting vocal cords) supplying wide diamond-shaped opening of the glottis.
If posterior cricoarytenoids are paralyzed, the adductor muscles (of vocal cords) take the upper hand and the man might die because of lack of air. Therefore the posterior circoarytenoid muscles are termed safety muscles of the larynx.
Nerve Supply
All the intrinsic muscles of the larynx are supplied by recurrent laryngeal nerve with the exception of cricothyroid that is supplied by the external laryngeal nerve.
Clinical Significance
Damage of external laryngeal nerve: If it’s damaged, there’s some weakness of phonation as a result of decrease of tightening effect of cricothyroid muscle on the vocal cords.
Damage of recurrent laryngeal nerve: It’s frequently damaged, accidently during partial thyroidectomy:
- If damaged unilaterally, the vocal cord on the affected side is located in paramedian position (between abduction and adduction) and doesn’t vibrate. But, generally the other cord has the capacity to compensate and the phonation isn’t substantially changed. The sound (normal) generated by vocal cords move freely and even cross the midline to meet the paralyzed vocal cord.
- If damaged bilaterally, both the vocal cords is located in the paramedian position with consequent reduction of phonation and trouble in breathing.
Damage of both recurrent and external laryngeal nerves: If the recurrent and external laryngeal nerves are involved on either side, the vocal cords are farther abducted and repaired as a result of paralysis of all intrinsic muscles of the larynx. This is called the cadaveric position of vocal cords or rima glottidis.
Key Points
Exceptions:
- The cricothyroid is the only muscle being located on the outer aspect of the larynx.
- All the intrinsic muscles of the larynx are matched with the exception of transverse arytenoid (interarytenoid) that is unpaired.
- All the intrinsic muscles of larynx adduct the vocal cords with the exception of posterior cricoarytenoids, which abduct the vocal cords.
- All the intrinsic muscles of the larynx are matched with the exception of transverse arytenoid that is unpaired.
The student do not need to remember the origin and insertion of all the intrinsic muscles. Yet, they ought to understand about a couple of muscles in detail. All these are described in subsequent text.
Origin and Insertion of Muscles of The Larynx
CavityIt stretches from inlet of larynx, where it interacts with the lumen of laryngopharynx to the lower border of the cricoid cartilage, where it is continuous with the lumen of the trachea. The anterior wall of laryngeal cavity is longer in relation to the posterior wall. Laryngeal inlet is obliquely set, sloping downwards and backwards. It opens into the laryngopharynx. Borders
Inside the laryngeal cavity, 2 pairs of folds of the mucous membrane go (on every side) posteroanteriorly from arytenoid cartilage to the thyroid cartilage:
Clinical SignificanceLaryngeal obstruction: The mucous membrane of the superior part of larynx is extremely sensitive. When foreign body (a slice of food or a drop of water etc.) enters into the laryngeal inlet it causes immediate explosive coughing and the foreign body is expelled out. If this reflex is impeded or absent as in neurological lesion or after consuming alcohol, a foreign body (example, piece of meat) may goes into the laryngeal cavity and cause choking (i.e., laryngeal obstruction). Choking by food is a familiar cause of laryngeal obstruction and asphyxia. If foreign body isn’t dislodged and expelled out instantaneously by Heimlich maneuver, man will die inside minutes, just about certainly before there’s time to take him to the hospital. The Heimlich maneuver is done as follows: Stand behind the casualty, pass your arms under his arms, place hands in front of the casualty’s epigastrium with 1 hand created into a fist and the other hand being located over it. Now give three or four abdominal thrusts pointed upwards and backwards. By doing this, the remaining air in the lungs is squeezed upwards in trachea and larynx with power, dislodging foreign body and therefore alleviating laryngeal obstruction (choking). The foreign body is either expelled itself or removed. Subdivisions of the Laryngeal CavityThe laryngeal cavity is split into 3 parts by 2 pairs of vestibular and vocal folds, viz.
The aryepiglottic folds divide the vestibule from piriform recesses. Ventricle or sinus of the larynx (glottic compartment):
Clinical SignificanceLaryngocele: If air pressure in the laryngeal sinus is increased too much as in trumpet musicians, glass blowers or weight lifters the saccule dilates to create an air filled cystic swelling referred to as laryngocele. The laryngocele may be internal, when it’s found inside the larynx or external, when distended saccule herniates via the thyrohyoid membrane and comes outside the larynx. Mucous MembraneThe mucous membrane of the larynx is loosely connected, with the exception of over the posterior outermost layer of the epiglottis, true vocal cords, corniculate and cuneiform cartilages where it’s firmly adherent. The entire of the laryngeal cavity is lined by ciliated columnar epithelium with the exception of the anterior surface and upper half of the posterior surface of the epiglottis, upper parts of aryepiglottic folds and vocal folds that are lined by strati-fied squamous epithelium. The mucous glands are dispersed all over the mucous lining. They’re especially numerous on the posterior outermost layer of the epiglottis, posterior parts of aryepiglottic foldsand in the saccules. There aren’t any mucous glands in the vocal folds. Clinical SignificanceThe mucosa (lined by stratified squamous epithelium) lining the vocal cords is securely stuck to the vocal ligaments and there isn’t any interceding submucosa. This accounts for the pearly white avascular look of vocal cords. The edema of larynx doesn’t include the true vocal cords since there isn’t any submucous tissue. Nerve Supply of the Larynx
Clinical SignificanceIf internal laryngeal nerve is damaged, there’s anesthesia of the mucous membrane in the supraglottic portion and loss of protective cough reflex. Consequently, the foreign bodies can easily goes into the larynx. Arterial Supply of the LarynxThe arterial supply of larynx is as follows:
Venous Drainage of the LarynxThe veins draining the larynx follow the arteries. Theseare:
Lymphatic Drainage of the LarynxThe lymphatics from:
Rima Glottidis and PhonationIt’s the narrowest anteroposterior cleft of the laryngeal cavity. The anteroposterior diameter of glottis is 24 mm in adult males and 16 millimeters in adult females. Bounds
Subdivisions of Rima GlottidisThe rima glottidis is split into the following 2 parts:
Shape of Rima GlottidisThe size and shape of glottis changes with the movements ofthe vocal cords: In quiet breathing, the intermembranous part is triangular and intercartilaginous part is rectangular. As a whole the glottis is pentagonal. In complete divine guidance, the glottis widens and becomes diamond shaped as a result of abduction of vocal cords. During high pitched voice, the rima glottidis is reduced to a linear chink, because of adduction of both intermembranous and intercartilaginous parts. During whispering, the intermembranous part is exceptionally adducted and intercartilaginous part is divided by triangular gap, so leaving an inverted funnel shape to the rima glottidis. Clinical SignificanceLaryngoscopyThe inside of the larynx can be inspected directly by laryngoscope (direct laryngoscopy), or indirectly via a laryngeal mirror (indirect laryngoscopy). These structures are seen:
Mechanism of PhonationThe phonation (language) is generated by the vibrations of thevocal cords. The larger the amplitude of oscillation, thelouder is the sound. The larynx is similar to a wind instrument. The voice is produced in following way:
Key Points The vowels are voiced in the larynx because of vibration of vocal folds on the other hand consonants are generated by the intrinsic muscles of the tongue. The loudness of sound is dependent upon the amplitude of vibrating vocal folds, on the other hand pitch is dependent upon the frequency with which the vocal folds vibrate. Since the vocal cords are often longer in males than females, they vibrate with greater amplitude but with lower frequency. Therefore voice of male is louder but low pitched. Clinical SignificanceVocal Nodules (Vocalist’s or Screamer’s Nodules)During shaking the area of maximum contact between the vocal cords is right at the junction of their anterior one-third and posterior two-third and so subject to maximum friction. For this reason in people, who overuse their voice, like teachers, pop vocalists, the inflammatory nodules develop at these sites named vocal nodules. They can be bilateral andsymmetrical and change in size from that of pin head to a split pea. In early periods, they’re soft, reddish and edematous but afterwards become greyish or whitish in color. Rate this Article:   (72 votes, average: 4.32 out of 5) (72 votes, average: 4.32 out of 5)Trusted By The World’s Best |
|---|