The Pancreas is a soft, delicately lobulated, elongated exo-endocrine gland. It is formed of basically 2 parts: the Exocrine and the Endocrine. The exocrine part secretes the pancreatic juice and the endocrine part secretes the hormones, viz., insulin, etc. The pancreas (in Greek pan: all 1 kreas: flesh) gets its name due to its fleshy look.

Pancreas
The pancreatic juice is helpful in the digestion of lipids, carbohydrates, and proteins, while the pancreatic hormones keep glucose homeostasis.
Size and Shape

Pancreas: Shape and Size
- The pancreas is “J” shaped or retort-shaped being set obliquely. The bowl of retort represents its head and the stalk of retort represents its neck, body, and tail. Its measurements are:
- Length: 12-15 cm
- Width: 3-4 cm
- Thickness: 1.5-2 cm
- Weight: 80-90 grams
Location
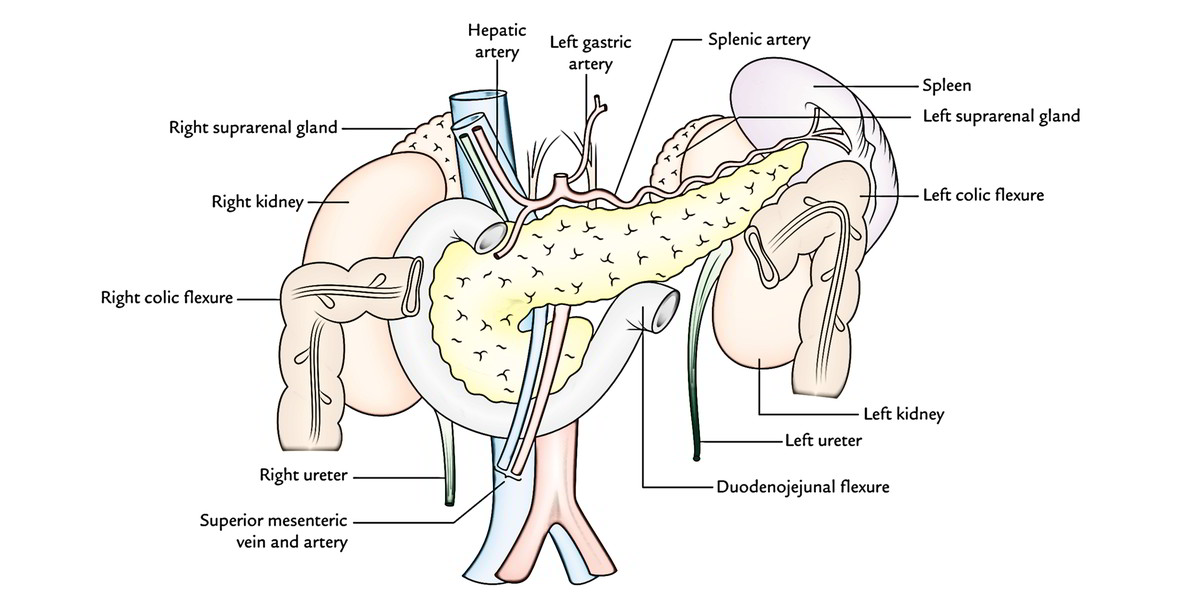
The pancreas is located more or less horizontally on the posterior abdominal wall in the epigastric and left hypochondriac regions. It crosses the posterior abdominal wall obliquely from concavity of the duodenum to the hilum of spleen opposite the level of T12-L3 vertebrae.
The greater part of the gland is retroperitoneal behind the serous floor of the lesser sac. Its left extremity- the tail, is located in the lienorenal ligament.
Parts (Subdivisions) and Relationships
For illustrative purposes, the pancreas is subdivided into 4 parts:
- Head (with 1 process- uncinate process).
- Neck.
- Body (with 1 process- tuber omentale).
- Tail.
Head of The Pancreas
The pancreas is deeply situated in the upper part of the abdomen, and concealed by many organs, for this reason not reachable for physical examination.
It’s the enlarged, disk -shaped right end of the pancreas, which is located in the concavity of the C-shaped duodenal loop in front of the L2 vertebra.
External Features
The head presents the following external features:
- 3 edges: Superior, inferior, and right lateral.
- 2 surfaces: Anterior and posterior.
- 1 process: Uncinate process. (It’s a hook like process from the lower and left part of the head. It goes toward the left behind the superior mesenteric vessels.).
Relations
Superior border is related to:
- first part of the duodenum, and.
- superior pancreatic duodenal artery.
Inferior border is related to:
- third part of the duodenum, and.
- inferior pancreatic duodenal artery.
Right Lateral border is related to:
- 2nd part of the duodenum, and.
- anterior and posterior pancreatic duodenal arterial arcades.
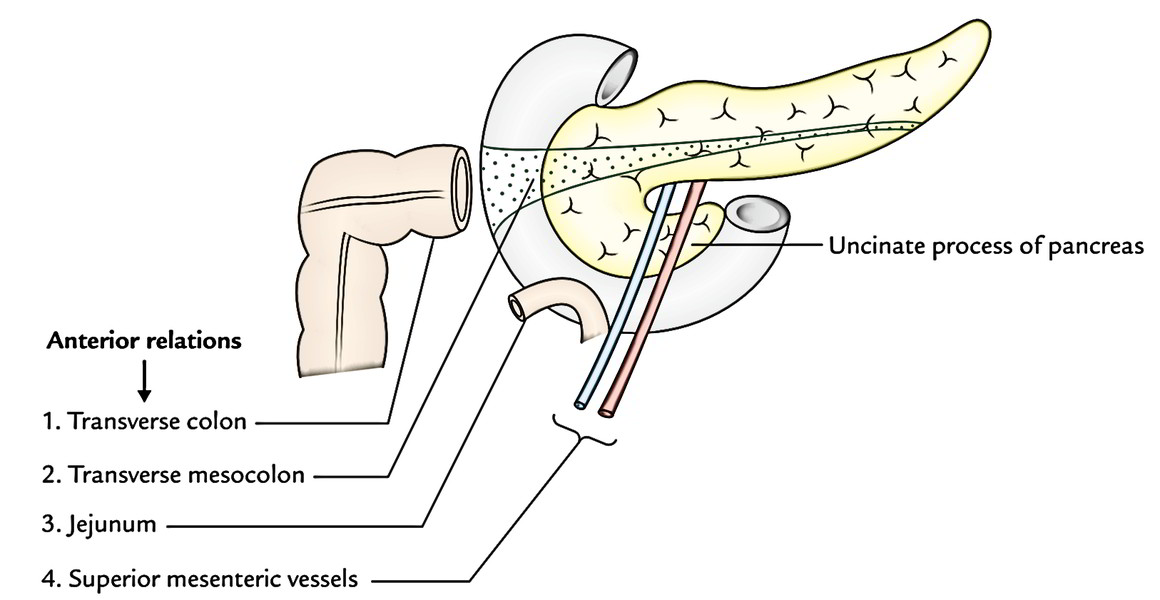
The anterior surface is associated from above downward to:
- gastroduodenal artery,
- transverse colon,
- root of the transverse mesocolon, and.
- jejunum.

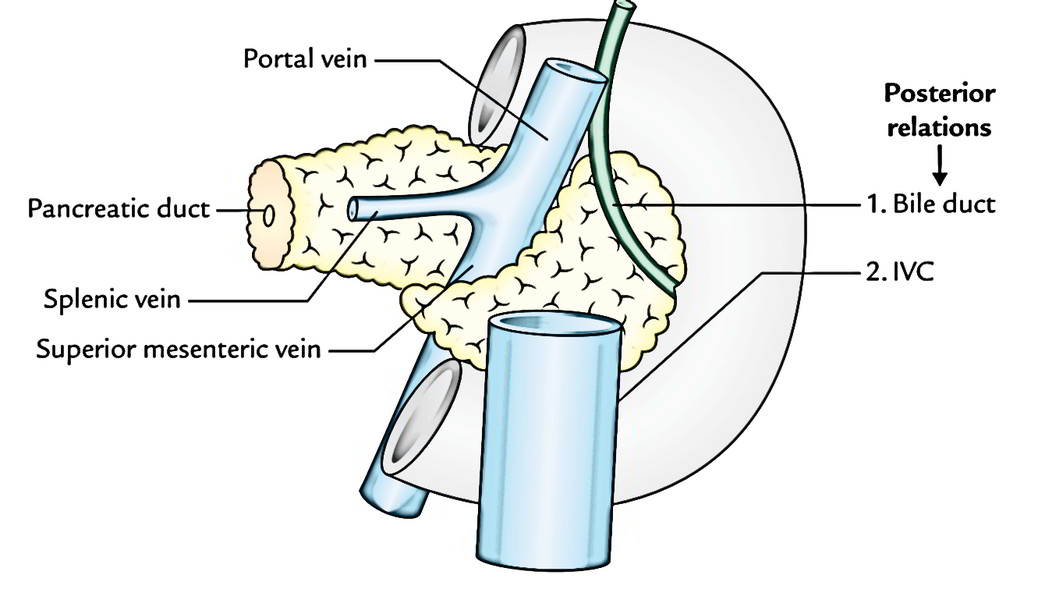
Posterior surface is related to:
- IVC,.
- left renal vein,.
- bile duct (being located in a groove, and might be seen embedded in the pancreatic tissue), and.
- right crus of diaphragm.
Uncinate process is related to:
- Anteriorly to superior mesenteric vessels, and.
- Posteriorly to the abdominal aorta.
Clinical Significance
Close relationship of the bile duct to the head of pancreas clarifies the incidence of jaundice from biliary retention in pancreatitis or tumor of the head of pancreas.
In half of the cases, the gallbladder is distended with bile, and palpable on physical examination.
Neck of The Pancreas
It’s a somewhat constricted part of the gland which connects the head together with the body. It’s about 2.5 cm (1 inch) long andis directed forwards, upward, and to the left.
External Features
It presents the following external features:
- 2 surfaces: Anterior and posterior.
- 2 edges: Upper and lower.
Relations
- Anterior surface is related to pylorus.
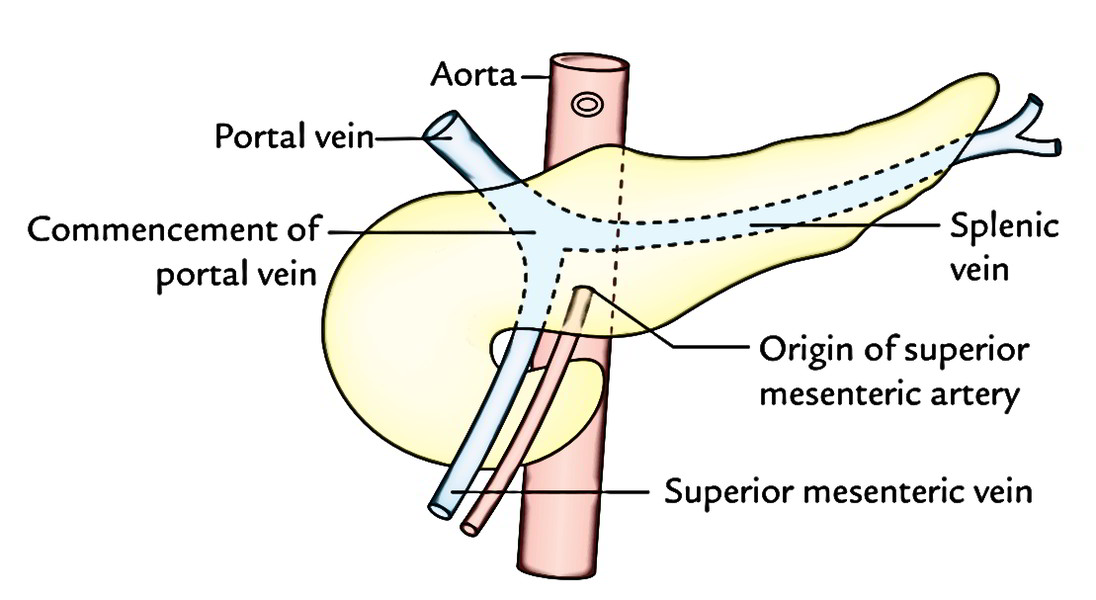
- Posterior surface is related to commencement of the portal vein.
- Upper border is related to the initial part of the duodenum.
- Lower border is related to the root of the transverse mesocolon.
Body of The Pancreas
- It’s the elongated part of the gland going from its neck to the tail.
- It enters toward the left of midline with a small upward and backward inclination.
- It is located in front of the vertebral column at or just below the transpyloric plane.
External Features
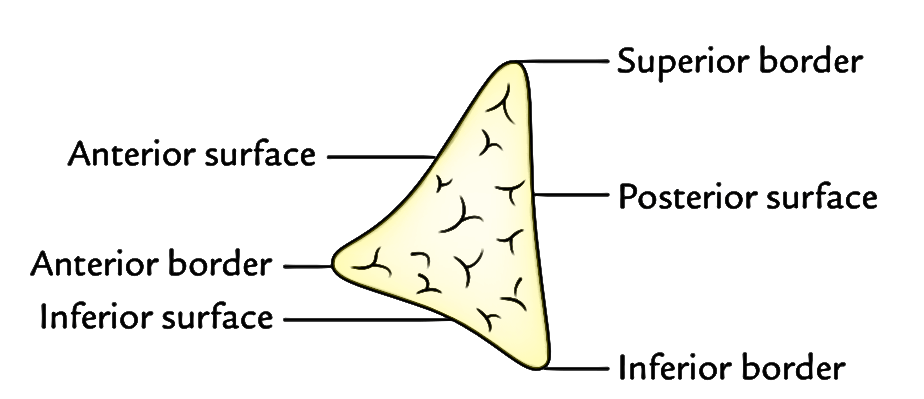
It’s somewhat triangular in cross section and gifts:
- 3 edges: Anterior, superior, and inferior.
- 3 surfaces: Anterior, posterior, and inferior.
- 1 process: Tuber omentale (a part of the body projects above the smaller curvature of the stomach and comes in touch together with the lesser omentum across the lesser sac).
Relations
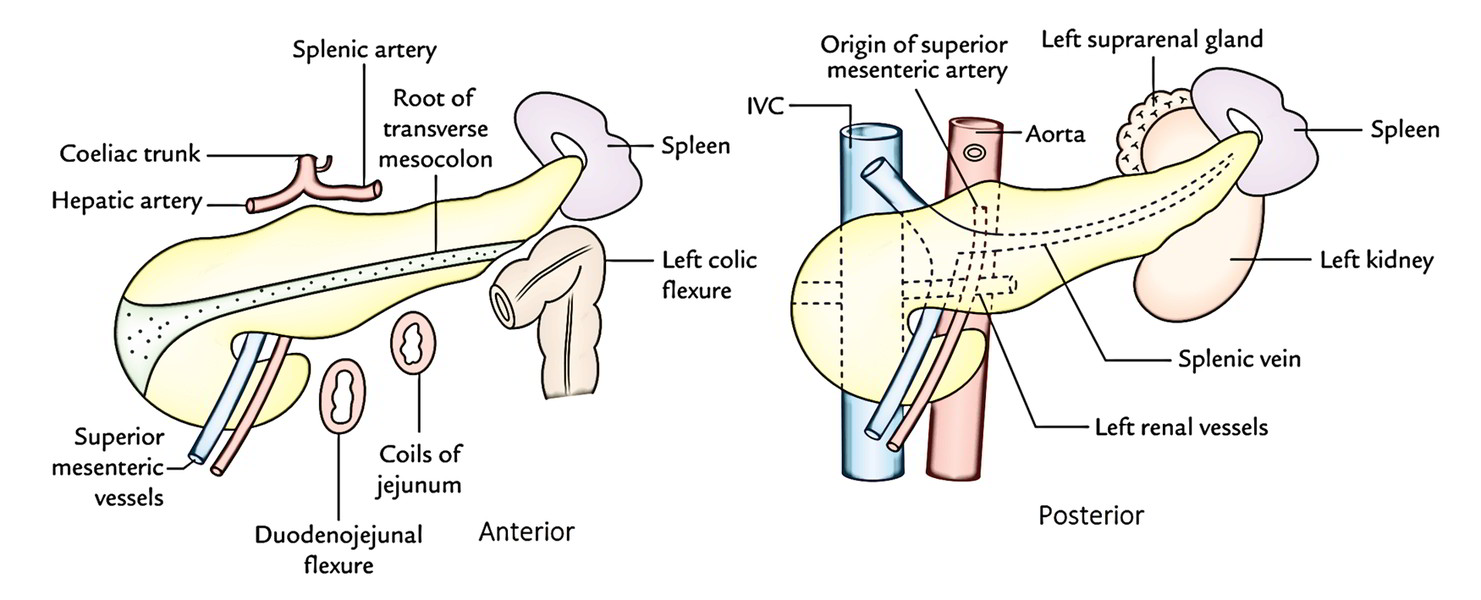
Anterior border supplies the connection to the root of transverse mesocolon.
Superior border is related to the coeliac artery above the tuber omentale, hepatic artery to the right, and splenic artery to the left of tuber omentale.
Inferior border is related to superior mesenteric vessels (at its right end).
Anterior surface (concave and directed forward and upward) is related to:
- lesser sac, and.
- stomach.
Posterior surface (devoid of peritoneum) is related to:
- aorta and origin of the superior mesenteric artery,
- left kidney and left suprarenal glands, and
- splenic vein generally is located in a groove below the level of the splenic artery.
Inferior surface (covered by peritoneum) is related to:
- duodenojejunal flexure, coils of jejunum, and.
- left colic flexure.
The tail of The Pancreas
- It’s the narrow left extremity of the pancreas.
- It is located in the lienorenal ligament alongside splenic vessels.
- It’s mobile unlike the other major retroperitoneal parts of the gland.
- It includes the largest number of islets of Langerhans per unit of tissue as compared to different parts of the gland.
Relations
All these are associated with the visceral surface of spleen between gastric feeling and colic opinion.
Ducts of The Pancreas
Normally there are 2 ducts: chief and accessory, which drain the exocrine secretion into the duodenum.
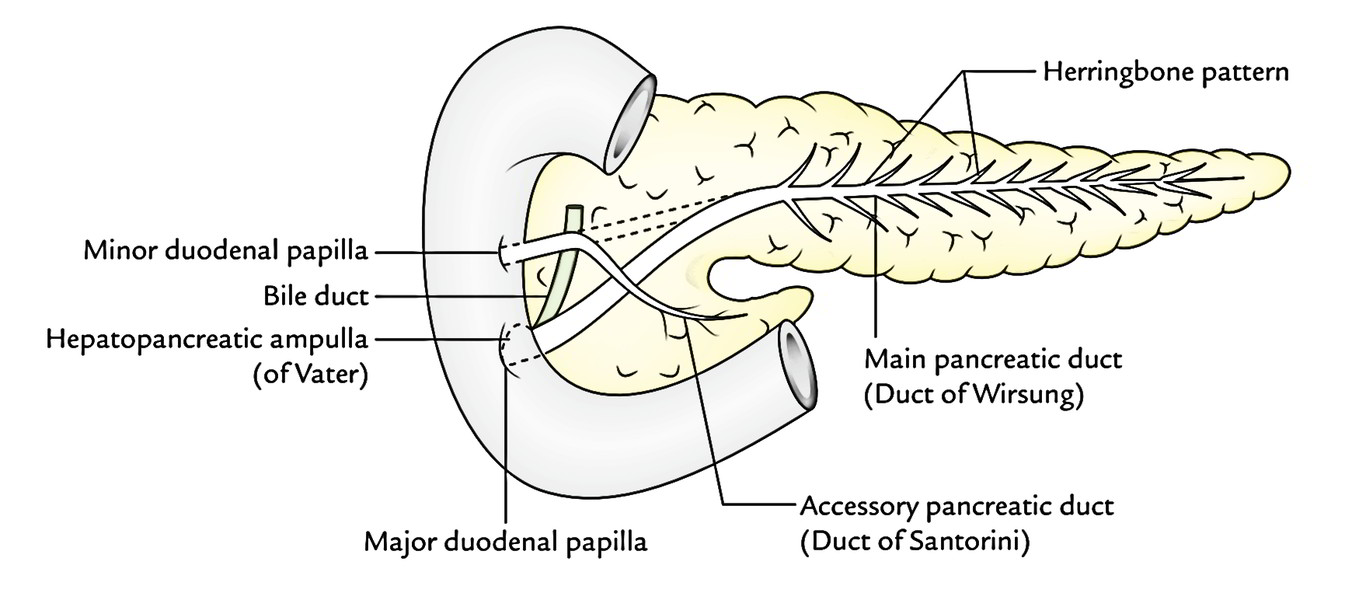
Primary Pancreatic Duct (of Wirsung)
- It starts in the tail and traverses the entire length of the gland near its posterior surface.
- At the neck, it turns downward, and after that to the right to goes into the 2nd part of duodenum.
- It joins the bile duct as it pierces the duodenal wall to create the hepatopancreatic ampulla (of Vater) which opens by a narrow mouth on the peak of major duodenal papilla 8-10 cm distal to the pylorus.
It gets tributaries (smaller ducts) throughout its length, at right angle to its long axis in a “herringbone pattern”.
It’s the only duct in 90% of cases.
Accessory Pancreatic Duct (of Santorini)
- It starts in the lower part of the head, and after that runs upward and medially, crossing in front of main pancreatic duct.
- It opens into the 2nd part of the duodenum on the peak of small duodenal papilla about 2-3 cm above the opening of main pancreatic duct (6-8 cm distal to pylorus).
- In 40% of cases, it interacts with all the primary duct while crossing it.
Development
The pancreas grows from 2 different buds: the ventral pancreatic bud and the dorsal pancreatic bud, therefore it got 2 ducts.
- The smaller ventral pancreatic bud appears in common with hepatic bud for the liver (later the bile duct).
- The bigger dorsal pancreatic bud appears more proximally, directly from the duodenum.
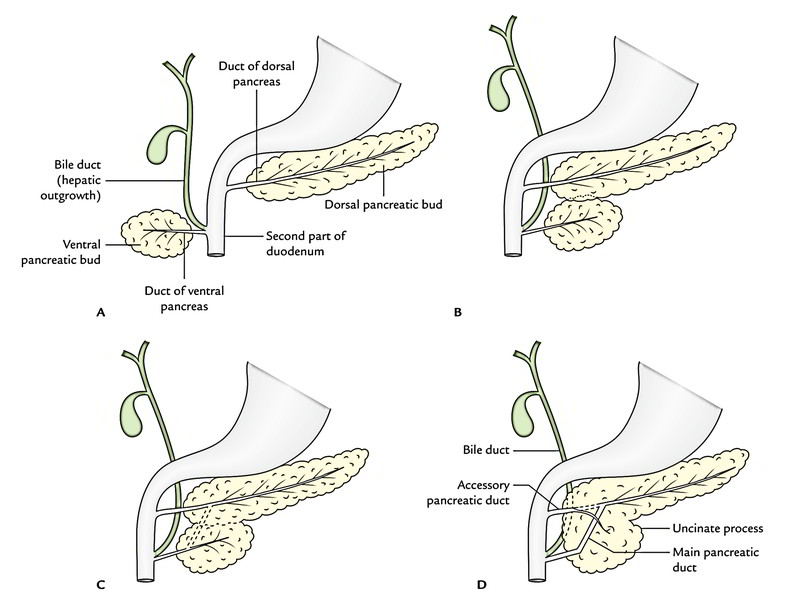
Following rotation of the gut, the ventral pancreatic bud (which creates the posterior part of the head and uncinate process) enters together with the bile duct into the position dorsal to the dorsal pancreatic bud (which creates the staying whole part of the gland). Both buds now fuse and their ducts anastomose with every other in this kind of style the duct of ventral pancreas creates the proximal part of the principal pancreatic duct while the duct of dorsal pancreas creates the rest distal part of the pancreatic duct. The proximal part of the dorsal pancreatic duct between the anastomosis and duodenum stays narrow and creates the accessory pancreatic duct. It generally interacts together with the main pancreatic duct.
Congenital Anomalies
- Annular pancreas is a developmental anomaly where a ring of pancreatic tissue encircles the next part of the duodenum.
- Accessory pancreatic tissue could be seen in (a) stomach wall, (b) duodenum (most common), (c) small intestine, (d) Meckel’s diverticulum, (e) greater omentum, and (f) hilum of spleen. It appears in the create of yellowish, lobulated nodules, generally single (1-6 millimeters) in diameter; about 1-third of these nodules include islets of Langerhans.
Arterial Supply
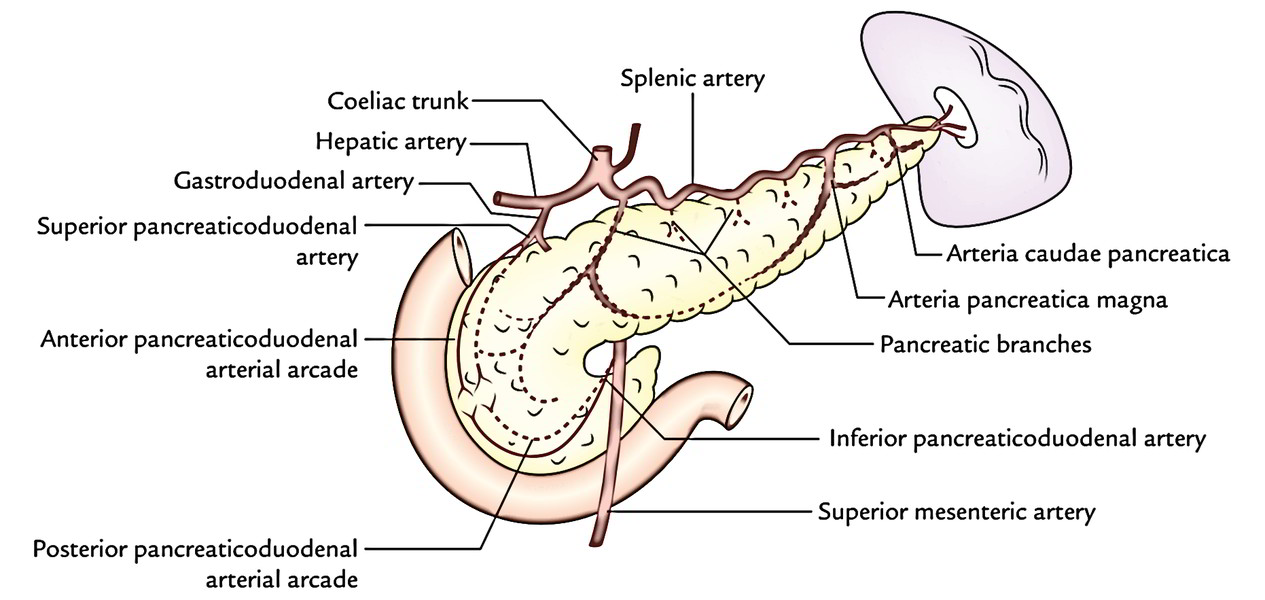
The pancreas is a high vascular structure and supplied by these arteries:
- Splenic artery, a branch of coeliac trunk: The splenic artery is the branch of coeliac trunk and it’s the primary source of blood supply to the pancreas. Its branches supply the body and tail of pancreas. 2 branches are called. 1 large branch which originates near the tail and runs toward the neck is known as arteria pancreatica magna. Another comparatively small branch, which runs toward the tip of the tail, is referred to as arteria caudae pancreatica.
- Superior pancreaticoduodenal artery: The superior pancreaticoduodenal arteryis a branch of gastroduodenal artery.
- Inferior pancreaticoduodenal artery: The inferior pancreaticoduodenal arteryis a branch of superior mesenteric artery.
Both the superior and inferior pancreaticoduodenal arteries divide into anterior and posterior branches, which run between the concavity of the duodenum and the head of pancreas. The anastomoses between anterior and posterior branches create anterior and posterior pancreaticoduodenal arterial arcades.
Since the pancreas grows at the junction of the foregut and midgut, it’s furnished by the branches of the artery of foregut (coeliac trunk) and the branches of the artery of midgut (superior mesenteric artery).
Venous Drainage
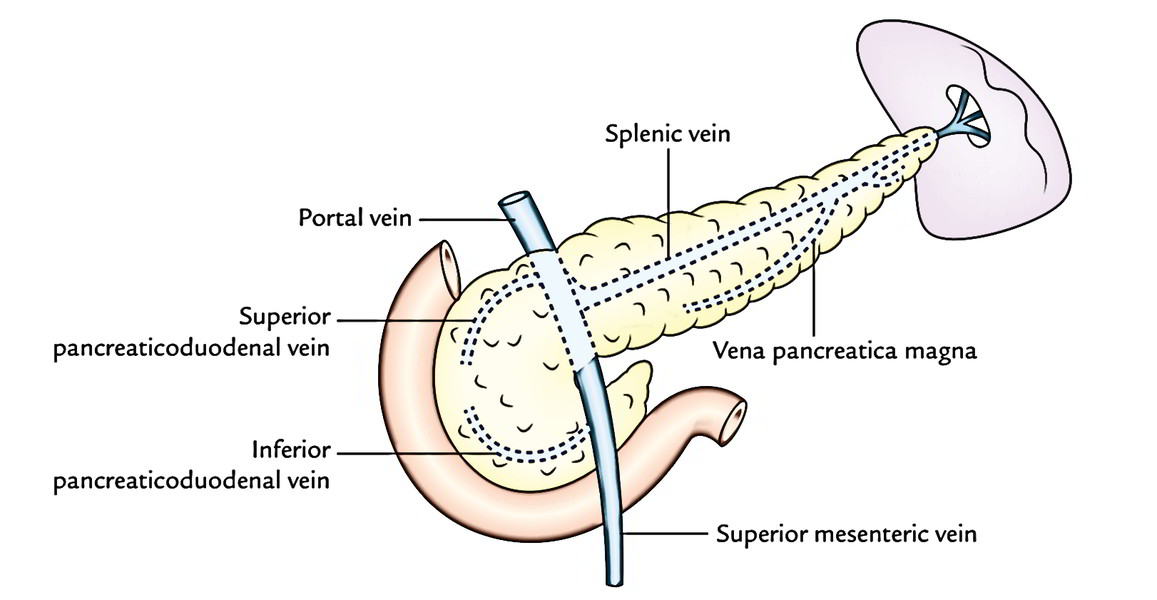
The veins of the pancreas drain into (a) portal vein, (b) superior mesenteric vein, and (c) splenic vein.
Lymphatic Drainage
The lymphatics from the pancreas follow the arteries and drain primarily into these groups of lymph nodes:
- Pancreaticosplenic nodes (primary group).
- Coeliac nodes.
- Superior mesenteric nodes.
- Pyloric nodes.
Nerve Supply
The sympathetic and parasympathetic nerve fibres reach the gland along its arteries from coeliac and superior mesenteric plexuses.
The sympathetic supply is vasomotor while the parasympathetic supply restrains the pancreatic secretion.
Control of Pancreatic Secretion
Pancreatic secretion, like gastric secretion, is controlled by both neural and hormonal mechanisms. Neural control is via parasympathetic axons. When parasympathetic nerve impulses activate the stomach mucosa, they also stimulate the pancreas to secrete pancreatic juice.
Hormonal control of pancreatic secretion results from two hormones that stimulate different types of pancreatic cells. Acid chyme entering the duodenum stimulates the intestinal mucosa to release the hormone secretin. Secretin is carried by blood to the pancreas, where it stimulates
secretion of pancreatic juice that is rich in bicarbonate ions. Bicarbonate ions neutralize the acidity of the chyme entering the small intestine. Lipid-rich chyme stimulates production of cholecystokinin by the intestinal mucosa. CCK stimulates secretion of pancreatic juice that is rich in digestive enzymes.
Hormones of The Pancreas
| Hormone | Control | Action | Disorders |
|---|---|---|---|
| Glucagon | Blood glucose level | Increases blood glucose by stimulating the liver to convert glycogen and other nutrients into glucose | |
| Insulin | Blood glucose level | Decreases blood glucose by aiding movement of glucose into cells and promoting the conversion of glucose into glycogen | Hyposecretion causes type I diabetes mellitus. Hypersecretion may cause hypoglycemia. |
Glucagon
Glucagon (glu’-kah-gon) increases the concentration of glucose in the blood. It does this by activating the liver to convert glycogen and certain noncarbohydrates, such as amino acids, into glucose. Glucagon helps to maintain the blood level of glucose within normal limits even when carbohydrates are depleted due to long intervals between meals. Epinephrine stimulates a similar action, but glucagon is more effective. Glucagon secretion is controlled by the blood level of glucose via a negative-feedback mechanism. A low level of blood glucose stimulates glucagon secretion, and a high level of blood glucose inhibits glucagon secretion.
Insulin
The effect of insulin on the level of blood glucose is opposite that of glucagon. Insulin decreases blood glucose by aiding the movement of glucose into body cells, where it can be used as a source of energy. Without insulin, glucose is not readily available to most cells for cellular respiration. Insulin also stimulates the liver to convert glucose into glycogen for storage. The antagonistic functions of glucagon and insulin maintain the concentration of glucose in the blood within normal limits. Like glucagon, the level of blood glucose regulates the secretion of insulin. High blood glucose levels stimulate insulin secretion; low levels inhibit insulin secretion.
Disorders Diabetes mellitus (d–-ah-be i-tez mel-li i-tus) is caused by the hyposecretion of insulin or the inability of target cells to recognize it due to a loss of insulin receptors. Type I or insulin-dependent diabetes is an autoimmune metabolic disorder that usually appears in persons less than 20 years of age. For this reason, it is sometimes called juvenile diabetes, although the condition persists for life. Type I diabetes results when the immune response destroys the beta cells in pancreatic islets. Because the metabolism of carbohydrates, fats, and proteins is affected, persons with type I diabetes must follow a restrictive diet. They must also check their blood glucose level several times a day and inject themselves with insulin, or receive insulin from an implanted insulin pump, to keep their blood glucose concentration within normal limits.
The vast majority of diabetics have type II or insulin- independent diabetes, which is caused by a reduction of the insulin receptors on target cells. This form of diabetes, also called adult-onset diabetes, usually appears after 40 years of age in persons who are overweight. The symptoms are less severe than in type I diabetes and can be controlled by a careful diet and oral medications that help regulate blood levels of glucose. The current increase in obesity among children and young adults is of concern because it may lead to an increase in type II diabetes. In either case, the result is hyperglycemia, excessively high levels of glucose in the blood. With insufficient insulin or a reduction in target insulin receptors, glucose cannot get into cells easily, and cells must rely more heavily on triglycerides as an energy source for cellular respiration. The products of this reaction tend to decrease blood pH (acidosis), which can inactivate vital enzymes and may lead to death.
An excessive production of insulin, or overdose of insulin, may lead to hypoglycemia, a condition characterized by excessively low blood glucose levels. Symptoms include acute fatigue, weakness, increased irritability, and restlessness. In extreme conditions, it may lead to an insulin- triggered coma.
Clinical Significance
- Carcinoma of the head of pancreas is common. It compresses the bile duct resulting in consistent obstructive jaundice. It might press the portal vein or may include the stomach because of shut area of these structures to the head of pancreas.
- Acute pancreatitis is the extreme inflammation of the pancreas. It takes place because of obstruction of pancreatic duct, ingestion of alcohol, viral infections (mumps), or trauma. It’s serious affliction because activated pancreatic enzymes leak into the substance of pancreas and begins the autodigestion of the gland. Medically, it presents as quite acute pain in the epigastric region radiating to the back, temperature, nausea, and vomiting. The serum amylase, level is increased 4 times.

 (62 votes, average: 4.50 out of 5)
(62 votes, average: 4.50 out of 5)