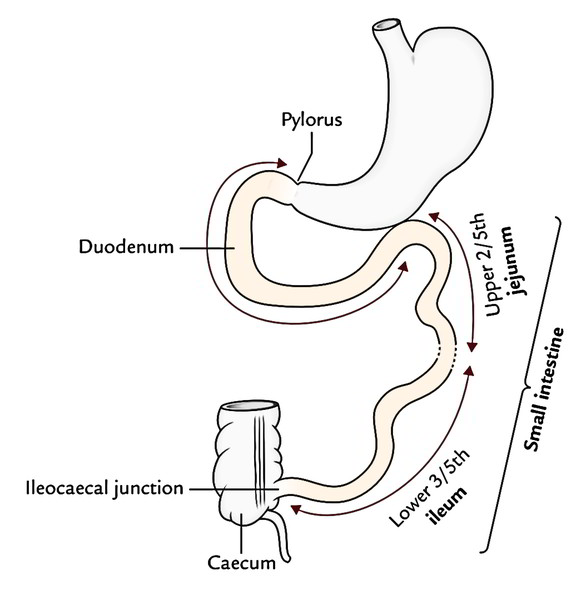
The Small Intestine is a winding, tightly-folded tube in the digestive system that absorbs about 90% of the nutrients from the food we eat. Anatomy says, the small intestine extends from the pylorus to the ileocaecal junction. Its length goes about 6 m and is also divided into 3 parts: duodenum, jejunum, and ileum. The duodenum is the proximal fixed part that is about 10 inches (25 cm) long. The other 2 parts, i.e., jejunum and ileum are freely mobile and stays long.
The duodenum mostly remains retroperitoneal and fixed. It gets chyme from the stomach, bile from the gallbladder, and pancreatic juice from the pancreas. The fixation of duodenum is important because mobile duodenum will cause twisting and kinking of common bile duct (CBD) and pancreatic ducts which open into it. It’s closely connected with pancreas and extra hepatic biliary apparatus. Thus, medically it’s regarded as another thing.
The jejunum and ileum are largely concerned with the digestion and absorption of digested food; for this reason these 2 parts together create the small intestine appropriate. This description of the small intestine is confined only to the jejunum and ileum.
Duodenum
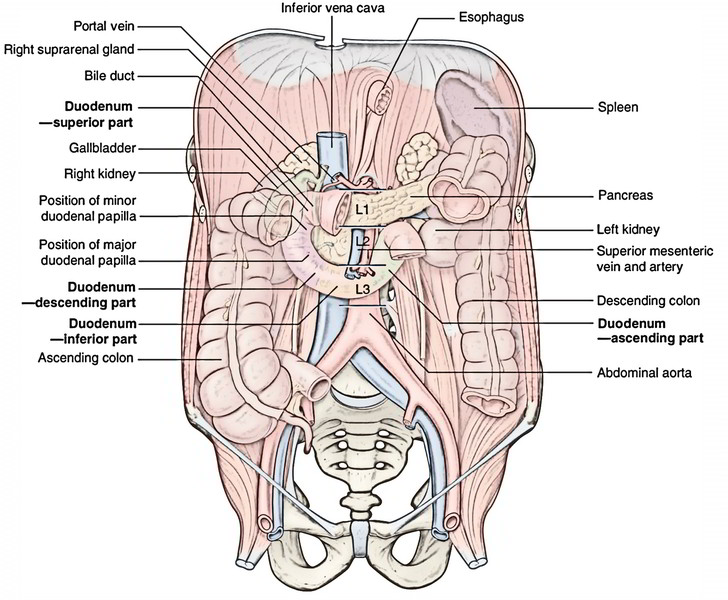
The frst part of the small intestine is the duodenum. This C-shaped structure, adjacent to the head of the pancreas, is 20 to 2 5 em long and is above the level of the umbilicus; its lumen is the widest of the small intestine. It is retroperitoneal except for its beginning, which is connected to the liver by the hepatoduodenal ligament, a partn of the lesser omentum.
Jejunum and Ileum
The small intestine suitable stretches from the duodenojejunal flexureto the ileocaecal junction. Its upper two fifth creates the jejunumand its lower 3-fifth creates the ileum. Nevertheless, there’s no clear line of demarcation. The jejunum and ileum are suspended from the posterior abdominal wall by a large fold of peritoneum known as the mesentery of small intestine; thus, the small intestine appreciates a substantial freedom. The structure of the small intestine corresponds to its functional demands.
Structure
The wall of the small intestine contains 4 layers. From inside outward, these are:
(a) mucosa, (b) submucosa, (c) muscle layer, and (d) serosa.
Mucosa
The mucosa presents the subsequent 3 important features.
- Larger Surface Area: For digestion and absorption of nutriments, the surface area of mucus membrane is extremely improved by plicae circulares, villi, and microvilli.
- Plicae circulares (or valves of Kerckring): All these are circular folds, that are long-lasting and aren’t obliterated by distension.
- Villi: The surface of circular folds is thrown into small (0.5 mm or less in length) finger like projections named villi.
- Microvilli: The surface epithelium covering the villi presents microvilli (or striated border).
Points to be noticed
- The overall surface area of mucosa of the small intestine is all about 200 m2.
- The whole epithelial lining of the small intestine is replaced in every 2 to 4 days.
Intestinal Glands (Crypts of Lieberkuhn).
Between the bases of villi, the epithelium is invaginated in the lamina propria to create intestinal glands. They secrete digestive enzymes and mucous.
Lymphatic Follicles.
The lamina propria of the mucous membrane includes 2 types of lymphatic follicles.
- Solitary lymph follicles: These are 1-2 millimeters in diameter and are spread through the length of the small intestine.
- Aggregated lymph follicles: They create circular or oval Positions named Peyer’s patches. Every Peyer’s patch is composed of about 260 solitary lymph follicles and its length varies from 2 to 10 cm. They’re present lengthwise along the antimesenteric border. Peyer’s patches are small, circular, and fewer in the distal part of the jejunum, and large, oval, and numerous in the ileum especially in its distal part. In the distal part of the ileum where Peyer’s patches are a lot bigger and most numerous may go in the submucosa after breaking the muscularis mucosa.
Submucosa
It’s created from loose areolar tissue and includes blood vessels, lymph vessels, and nerve plexus (Meissner’s plexus).
Muscle Layer
It’s created from outer longitudinal and inner circular layers of smooth muscle. Auerbach’s plexus of nerves is present between these 2 layers.
Serosa
It’s created by the visceral peritoneum and is lined by the simple squamous epithelium.
Clinical Significance
Typhoid And Tubercular Ulcers
Peyer’s patches may be felt via the antimesenteric border of the ileum. They may ulcerate in typhoid fever creating feature vertically oriented, oval ulcers which might occasionally perforate. Because of this, patients afflicted by typhoid fever are given hot soft diets.
After mending, the typhoid, ulcers don’t cause intestinal obstruction like tubercular ulcers. Notice, the tubercular ulcers are circularly put; therefore, after recovering they frequently cause constriction of the lumen of small intestine by fibrous tissue, resulting in Intestinal Obstruction.
Arterial Supply
The jejunum and ileum are supplied by the jejunal and ileal branches (12-15 in number) of the superior mesenteric artery they originate from the left side of the superior mesenteric artery and goes into the mesentery to reach the intestine the terminal part of the ileum is supplied by the ileal branches of the ileocolic branch of the superior mesenteric artery as soon as these goes into the mesentery they break up into smaller branches which anastomose with every other to create a series of arterial arcades that are more complex in the ileum than in the jejunum.
From the convexities of the endmost arcades, small parallel straight vessels named “vasa recta” originate and pass to the mesenteric border of the gut to be spread instead to the opposite surfaces of the small intestine. The anastomosis between the vasa recta is lousy.
Venous Drainage
The veins correspond to the branches of superior mesenteric artery and drain into the portal vein, which takes the products of protein and carbs to the liver.
Lymphatic Drainage
The lymph vessels from the small intestine go through a large number of mesenteric nodes (lymph nodes within the mesentery) and ultimately drain into superior mesenteric nodes present around the origin of superior mesenteric artery. The lymphatics of the small intestine have a circular course in its wall. The circular tubercular ulcers and following strictures in the small intestine are because of participation of these lymphatics in tuberculosis.
Nerve Supply
The small intestine is provided by both sympathetic and parasympathetic nerve fibres. The sympathetic supply is originated from T10 T11 spinal sections via splanchnic nerves and superior mesenteric plexus. Because of this, pain from the jejunum and ileum is referred to the umbilical region. The parasympathetic supply is originated from the vagus nerves via the coeliac and superior mesenteric plexuses.
The sympathetic fibres are motor to the gut-sphincters on the other hand the parasympathetic fibres stimulate the peristalsis and are inhibitory to the sphincters.
Mesentery of The Small Intestine
It’s a broad fan-shaped fold of the peritoneum, which suspends the small intestine (jejunum and ileum) from the posterior abdominal wall. It’s the root (connected margin) and free margin (intestinal margin). The root is connected to an oblique line across the posterior abdominal wall going from the duodenojejunal flexureto the ileocaecal junction.
The duodenojejunal flexure is located to the left side of 2nd lumbar vertebra, on the other hand ileocaecal junction is located at the right sacroiliac joint.
The root of mesentery is around 6 inches (15 cm) long while its free margin (periphery of the mesentery) is about 6 m long. This accounts for the creation of folds/ pleats in it (a frill-like arrangement resembling a full skirt).
Surface Marking of The Root of Mesentery
The point representing the duodenojejunal flexure is located 1 cm below the transpyloric plane and 2.5 cm to the left of midline. The point representing the ileocaecal junction corresponds to the point of intersection between right lateral and transtubercular planes.
Clinical Significance
- The great length of the mesentery enables the descent of the loop of small intestine into the sac of inguinal or femoral herniae.
- A group of lymph nodes when contaminated may become adherent to an adjoining loop of small intestine and can lead to the mechanical obstruction. An acute terminal mesenteric lymphadenitis is usually indistinguishable from an acute appendicitis.
- Mesenteric cyst: The mesentery is the site of cystic swellings which largely originate from the mesenteric lymph nodes. Medically, the mesenteric cyst shows as a painless, cystic fluctuant swelling in the umbilical region. On evaluation, the characteristic attribute of the swelling is that it’s more mobile in the way at right angles to the line of the connection of the mesentery and less mobile along the line of connection of the mesentery.
- The failure of root of mesentery to fuse over its whole length together with the posterior abdominal wall enables a pocket of the peritoneum to be created which may create a sac of an intraparietal hernia referred to as mesenteric parietal hernia of Waldeyer.
The differences between the duodenum and small intestine suitable (jejunum and ileum) are provided in the following box:
| Duodenum | Small intestine proper |
|---|---|
| Short in length (25 cm) | Long in length (<6 m) |
| Supplied by two rows of vasa recta | Supplied by single row of vasa recta |
| Presence of Brunner glands in submucus coat | Absence of glands in submucus coat |
Differences between the Jejunum and Ileum
Both jejunum and ileum have characteristic features which make them identifiable during procedure by the surgeons.
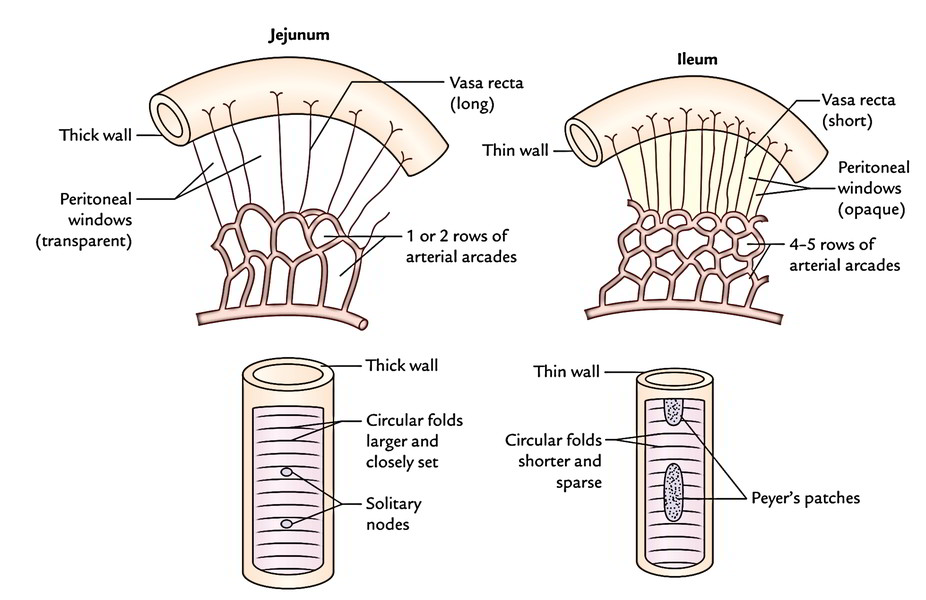
The jejunum is more vascular than the ileum and is somewhat wider in diameter compared to the ileum. It feels thicker between the finger and thumb in relation to the ileum, because its mucous membrane is thrown into more and closely place circular folds (plicae circulares). The ileum, on the flip side, possesses many more aggregated lymph follicles (Peyer’s patches) in its wall than jejunum.
Differences Between The Jejunum And Ileum
| Features | Jejunum | Ileum |
|---|---|---|
| Walls | Thicker and more vascular | Thinner and less vascular |
| Lumen | Wider and often found empty (diameter = 4 cm) | Narrower and often found full (diameter = 3.5 cm) |
| Circular folds/plicae circulares (valves of Kerckring) | Longer and closely set | Smaller and sparsely set |
| Villi | More, larger, thicker, and leaf-like | Less, shorter, thinner, and finger-like |
| Aggregated lymph follicles (Peyer’s patches) | Small, circular, and few in number, and found only in the distal part of the jejunum | Large oval and more in number (± 10 cm X 1.5 cm), and found throughout the extent of ileum being maximum in the distal part |
| Mesentery | Contains less fat and becomes semitranslucent between the vasa recta called peritoneal windows | Contains more fat and there are no peritoneal windows between the vasa recta |
| Arterial arcades | One or two rows with long vasa recta | Four or five rows with short vasa recta |
Development
The jejunum and ileum grow from the U shaped midgut loop having cephalic and caudal limbs. The cephalic limb provides rise to the jejunum and upper part of the ileum, and the caudal limb provides rise to the lower part of the ileum. In the embryonic life, the apex of the midgut loop interacts with the yolk sac via the vitello-intestinal duct. The vitelline duct is usually obliterated by the sixth week of intrauterine life.
Clinical Significance
Meckel’s Diverticulum (or Ileal Diverticulum)
Itis the continual proximal part of the embryonic vitello-intestinal duct. It presents the following characteristic features:
- It takes place in 2 percent of the themes.
- It’s generally 2 inches (5 cm) long.
- It’s situated about 2 feet (60 cm) proximal to the ileocaecal junction.
- It’s much more common in men.
- The calibre and structure of its wall are quite similar to that of the ileum.
- Its apex could be free or connected to the umbilicus by a fibrous band.
- It’s connected to the antimesenteric border of the ileum.
- It may include ectopic gastric mucosa and pancreatic tissue.
Normally, it’s symptomless but might cause the following clinical problems:
- It can cause intestinal obstruction.
- When it includes ectopic gastric mucosa or pancreatic tissue, its thin wall may ulcerate, perforate, and bleed to mimic the acute abdomen.
- When inflamed, its symptoms are like that of “acute appendicitis”.
Dictum: In a medically diagnosed case of acute appendicitis, if a healthy appendix is seen during procedure the surgeon should look for Meckel’s diverticulum.
Structure of Small Intestine
There are three sequential segments composing the small intestine. The duodenum (du-o-de ‘-num) is a very short section, about 25 to 30 cm long, that receives chyme from the stomach. The middle section is the jejunum (je-ju’-num), and it is about 160 to 200 cm long. The last and longest segment is the ileum (il’-e-um), which is about 170 to 215 cm long. The ileum joins with the large intestine at the ileal (il-e-al) orifice.
The small intestine is suspended from the posterior abdominal wall by the mesentery (mes ‘-en-ter-e), double folds of the peritoneum that provide support but allow movement. Blood vessels, lymphatic vessels, and nerves serving the small intestine are also supported by the mesentery.
The mucosa of the small intestine is modified to provide a very large surface area. The distinctive velvety appearance of the intestinal mucosa results from the presence of i ntestinal villi, tiny projections from the mucosa that are extremely abundant. Each villus is covered by simple columnar epithelium and contains a centrally located lacteal, a lymphatic capillary. A blood capillary network surrounds the lacteal. At the bases of the villi are tiny pits that open into intestinal glands, which secrete intestinal juice.
The mucosal surface area in contact with chyme and digestive fluids is further increased by the presence of numerous microvilli forming a “brush border”.
Intestinal Juice
The fluid secreted by the intestinal glands is known as intestinal juice. It is slightly alkaline and contains abundant water and mucus. Intestinal juice provides an appropriate environment for the action of bile salts and pancreatic digestive enzymes within the small intestine. Recall that trypsin in pancreatic juice is activated only after being mixed with intestinal secretions.
Regulation of Intestinal Secretion
The presence of chyme in the small intestine provides mechanical stimulation of the mucosa that activates the secretion of intestinal juice and enzymes. Chyme also causes an expansion of the intestinal wall, triggering a neural reflex that sends parasympathetic nerve impulses to the mucosa. The nerve impulses stimulate an increase in the rate of intestinal secretions.
Digestion And Absorption
Vigorous segmentation within the small intestine mixes chyme with bile, pancreatic juice, and intestinal juice. The emulsification of fats by bile and the continued digestion of carbohydrates, fats, and proteins by pancreatic and brush border enzymes occur within the small intestine. Brush border enzymes are embedded within the brush border of the small intestine mucosa. These actions complete the digestive process within the small intestine.
There are three brush border enzymes that split disaccharides into monosaccharides.
(1) Maltase converts maltose into glucose;
(2) sucrase converts sucrose into glucose and fructose; and
(3) lactase converts lactose into glucose and galactose.
Brush border enzymes acting on proteins are also present. Various peptidases split peptides into amino acids.
Summary of The Major Digestive Enzymes And Their Actions
| Enzyme | Substrate | Product |
| Saliva | ||
| Salivary amylase | Starch and glycogen | Maltose |
| Gastric Juice | ||
| Pepsin | Proteins | Peptides |
| Pancreatic Juice | ||
| Pancreatic amylase | Starch and glycogen | Maltose |
| Pancreatic lipase | Triglycerides | Monoglycerides* and fatty acids* |
| Trypsin | Proteins | Peptides |
| Brush Border Enzymes | ||
| Maltase | Maltose | Glucose* |
| Sucrase | Sucrose | Glucose* and fructose* |
| Lactase | Lactose | Glucose* and galactose* |
| Peptidases | Peptides | Amino acids* |
Carbohydrate digestion begins in the mouth and concludes in the small intestine. The end products of carbohydrate digestion are monosaccharides, the simple sugars glucose, fructose, and galactose. These sugars are absorbed across the epithelium and into the capillaries of the villi through both facilitated diffusion and active transport.
Fat (triglyceride) digestion primarily occurs in the small intestine. The end products are monoglycerides and fatty acids. Very small, or short-chain, fatty acids are absorbed by simple diffusion across the epithelium and into the capillaries of the villi. All other lipids require an alternate means of absorption. Bile salts interact to form structures called micelles, small transportation spheres that are hydrophilic on their surface and hydrophobic in their core. Micelles absorb large fatty acids, monoglycerides, cholesterol (a steroid), phospholipids, and lipid-soluble vitamins into their core and transport them to the intestinal brush border. The contents of the micelles move by simple diffusion into the epithelial cells. Once inside the epithelial cells, the fatty acids and monoglycerides recombine to form triglycerides. The triglycerides combine in small clusters with phospholipids, steroids, and lipid-soluble vitamins. These clusters are coated with protein and form structures known as chylomicrons (ki-lo-mi ‘-krons). The protein coat makes chylomicrons water-soluble. Chylomicrons move out of the epithelial cells by exocytosis and enter the lacteals of the villi. They are carried by lymphatic vessels to the left subclavian vein, where lymph from the intestine enters the blood.
Protein digestion begins in the stomach and concludes in the small intestine. The end products are amino acids, which are actively absorbed across the epithelium and into the capillaries of villi.
In addition to the end products of digestion, other needed substances are absorbed in the small intestine. For example, water, minerals, and water-soluble vitamins are absorbed into the capillaries of villi. Materials absorbed into the blood are carried from the intestines to the liver via the hepatic portal vein. After processing by the liver, appropriate concentrations of nutrients are released into the general circulation to serve the needs of tissue cells. In this way, the liver contributes to the overall homeostasis of the body.

 (50 votes, average: 4.68 out of 5)
(50 votes, average: 4.68 out of 5)