Location
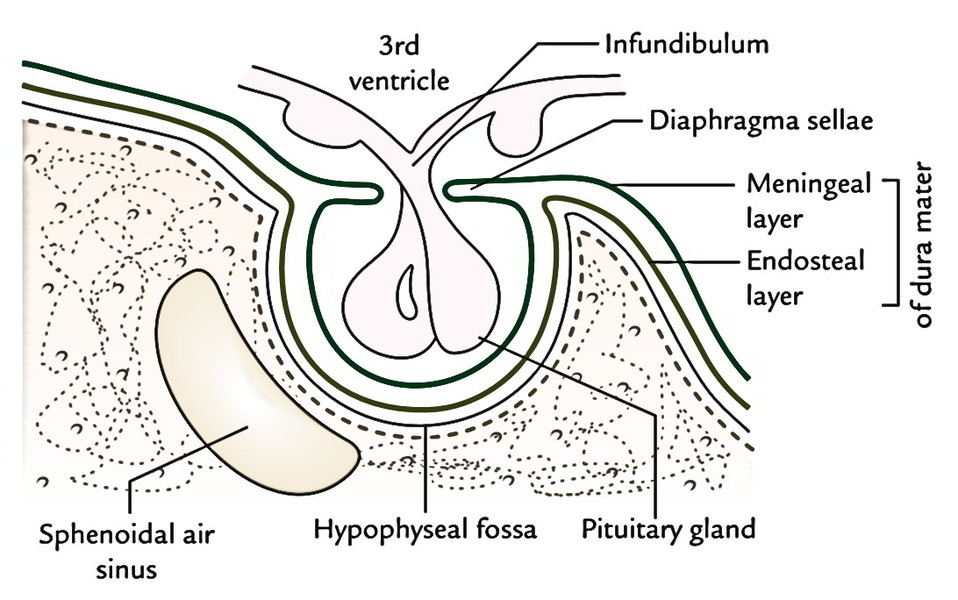
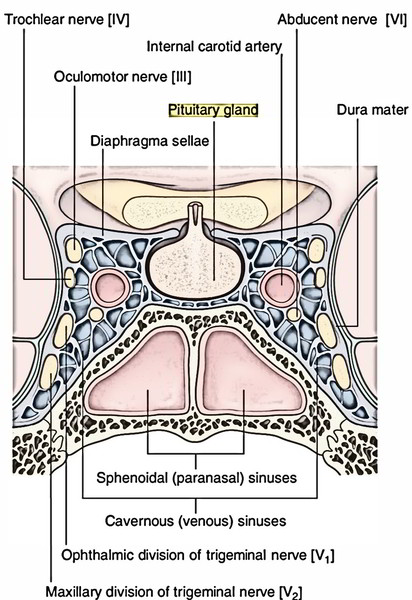
The pituitary gland is situated in the hypophyseal fossa on the superior outermost layer of the body of the sphenoid (sella turcica) and is a small endocrine gland Suspended from the floor of the 3rd ventricle of the brain by a narrow stalk referred to as infundibulum. The gland is enclosed in the dural sheath, where anxious upper wall the diaphragma sellae is perforated by the infundibulum or stalk. Pituitary gland is associated with the cavernous sinus and in front and behind to the anterior and posterior intercavernous sinuses, on every side.
Shape and Measurements
The gland is oval in shape and measures 8 millimeter antero-posteriorly, 12 mm transversely and weighs about 500 mg.
Connections
Superior: Optic chiasma with diaphragma sella interceding Inferior: Sphenoidal air sinuses with thin bony plate of the hypophyseal fossa interceding.
Lateral: Cavernous sinus on every side.
Subdivisions
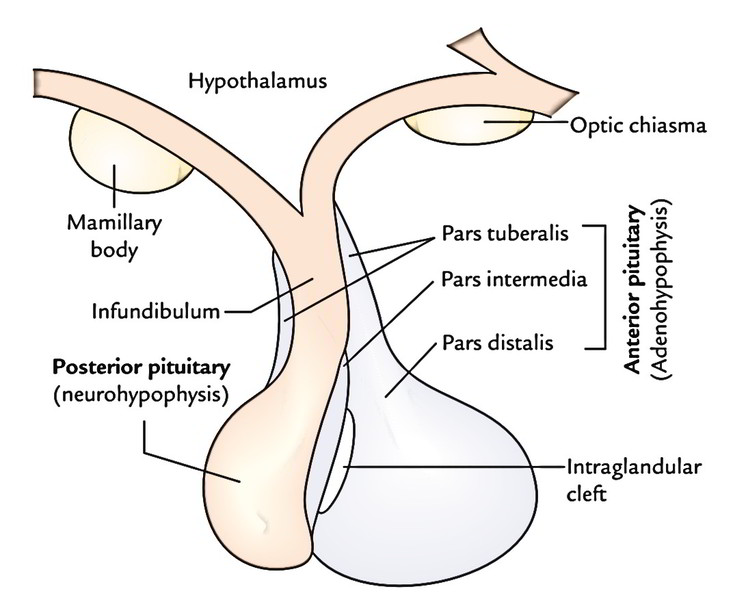
The gland has 2 principal subdivisions: adenohypophysis and neurohypophysis, which differ from every other embryologically, morphologically and functionally. The adenohypophysis grows as a diverticulum (Rathke’s pouch) from the ectodermal roof of the stomodeum. Normally the communication together with the roof of the pharynx goes away entirely owing to the rapid growth of the sphenoid. Sometimes, however, it might continue as a craniopharyngeal canal. The uppermost part of the initial diverticulum stays as a cleft which divides the pars anterior and pars intermedia. The neurohypophysis grows as a downgrowth from the floor of the diencephalon. Adenohypophysis is composed of:
- Pars anterior
- Pars intermedius
- Pars tuberalis
Neurohypophysis is composed of:
- Pars posterior
- Infundibulum
Functional Connections with Hypothalamus
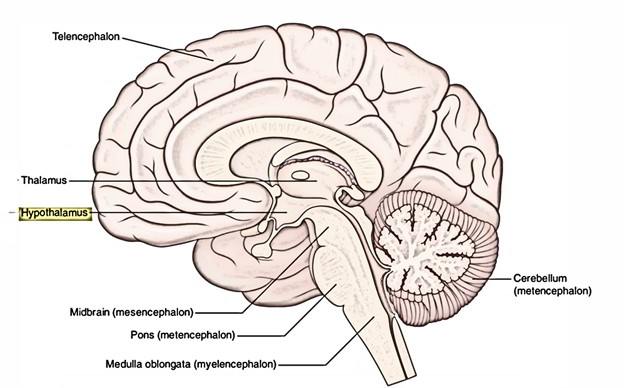
Hypothalamohypophysial Tract
It is composed of nerve fibres originating from the supraoptic and paraventricular nuclei of the hypothalamus and projecting into the posterior lobe of the pituitary gland The vasopressin and ADH generated in supraoptic and paraventricular nuclei are transported by the nerve fibres of the tract and saved in the nerve terminals (Herring bodies) of these fibres in the posterior lobe (neurohypophysis). Afterward hormones are released in the venous sinusoids as and when essential.
Hypothalamohypophysial Portal System
It includes 2 sets of capillaries-1 in the hypothalamus (median eminence) and the other in the hypophysis cerebri (sinusoids of pars anterior). The neurons of the hypothalamus create hormones-releasing factors in the capillaries of the median eminence and upper part of the infundibulum. All these are taken by the portal system to pars anterior where they excite it to discharge suitable hormones.
Arterial Supply
These branches of internal carotid artery supply the pituitary gland:
- Superior hypophyseal artery, 1 on every side.
- Inferior hypophyseal artery, 1 on every side.
Venous Drainage
Short veins from the pituitary gland drain into abutting dural venous sinuses (example, cavernous and intercavernous sinuses). The hormones pass out of the gland via venous blood to the goal sites.
Clinical Significance
Craniopharyngioma
The remnants of Rathke’s pouch may generate a tumor in the sphenoid bone referred to as craniopharyngioma.
Occasionally some cells of Rathke’s pouch go backwards along the roof of the nasopharynx and create an accessory lobe of the anterior lobe in the pharyngeal wall referred to as pharyngeal hypophysis.
Pituitary Tumors
The pituitary tumors take place generally. The commonest tumor of the pituitary gland is adenoma originating from its chromophobe cells. Pituitary adenoma generates 2 types of symptoms: (a) symptoms because of pressure on adjacent structures and (b) symptoms because of endocrine disruptions.
Symptoms because of pressure on adjacent structures:
- Enlargement of hypophyseal fossa because of downward increase (intrasellar increase) of an adenoma. It’s viewed as ballooning of hypophyseal fossa (sella turcica) in plane radiograph of skull (lateral view).
- Temple hemianopia (loss of vision in left and right temporal fields of vision) because of the upward development of adenoma pressing the central part of the optic chiasma.
- Exophthalmos and ophthalmoplegia on account of pressure on the cavernous sinus.
Symptoms because of endocrine perturbations:
- Gigantism before puberty and acromegaly in adults, because of excessive secretion of development (GH) hormone.
- Cushing syndrome because of excessive secretion ACTH.
- Dwarfism because of hyposecretion of GH in babies and children because of participation of the posterior lobe.
- Diabetes insipidus because of participation of the posterior lobe.
Surgical strategies for removal of pituitary adenoma: The pituitary tumors could be taken out by the transfrontal surgery or by the trans-sphenoidal route.
Trans-sphenoidal method: In this method, the surgeon enters the pituitary fossa from below via a sphenoidal air sinus, either via ethmoidal cells after lifting the periosteum from the medial wall of the orbit (actuallyit ought to be referred to as transorbital-transethmoidal trans-sphenoidal method) or by elevating the nasal mucosa from the nasal septum and removing the nasal septum (notice that nasal cavity itself isn’t entered) and rostrum of the sphenoid (transnasal-trans-sphenoidal method). Transfrontal (subfrontal) method: In this, the gland is approached via the anterior cranial fossa by elevating the frontal lobe of the brain.

 (52 votes, average: 4.48 out of 5)
(52 votes, average: 4.48 out of 5)