The Inferior Thoracic Aperture is broad and the upper part of the abdominal cavity is encompassed by the inferior thoracic aperture. The thoracic cavity and the abdominal cavity is divided by the large musculoaponeurotic diaphragm connected to the margins of thoracic outlet.
 Borders
Borders
 Borders
Borders- Anteriorly: Xiphisternal joint.
- Posteriorly: Body of 12th thoracic vertebra.
- Laterally: Costal margin and 11th and 12th ribs.
Diaphragm of inferior Thoracic Aperture
The thoracic outlet is closed by a large dome-shaped flat muscle named diaphragm. Because it separates thoracic cavity from abdominal cavity, it’s also named thoraco-abdominal diaphragm.
The diaphragm is the primary muscle of respiration. It’s dome shaped and is composed of peripheral muscular part, and central fibrous part named central tendon.
Origin
The origin of the diaphragm is split into 3 parts, viz.
- Sternal
- Costal
- Vertebral
Sternal Part
It is composed of 2 fleshy slides, which originate from the posterior surface of the xiphoid process.
Costal Part
On every side, it includes 6 fleshy skids, which originate from the inner surface of lower 6 ribs near their costal cartilages.
Vertebral Part
This part originates by means of
- Left and right crura of diaphragm
- 5 arcuate ligaments
Crura
- Right crus:
- It’s a vertical fleshy bundle, which originates from the right side of anterior aspects of the upper 3 lumbar vertebrae and intervening intervertebral discs.
- Left crus:
- It’s vertical fleshy bundle, which appears from the left side of anterior aspects of upper 2 lumbar vertebrae and the intervening intervertebral discs.
- The medial margins of the crura are tendinous.
Arcuate Ligaments
- Median arcuate ligament is an arched fibrous band extending between the upper ends of 2 crura.
- Medial arcuate ligament is the thickened upper margin of the psoas sheath. It stretches from the side of the body of L2 vertebra to the tip of the transverse process of LI vertebra.
- Lateral arcuate ligament is the thickened upper margin of fascia covering the anterior surface of the quadratuslumborum. It stretches from the tip of transverse process of LI vertebra to the 12th rib.
The right crus is connected to more number of vertebraebecause the right side diaphragm has to contract on themassive liver.
Insertion
From circumferential origin (vide supra), the muscle fibres converge in the direction of the central tendon and fit into its margins.
The features of the central tendon are as follows:
- It’s trifoliate in shape, having (a) an anterior (central) leaflet, and (b and c) 2 tongue shaped posterior leaflets. It resembles an equilateral triangle. The right posterior leaflet is short and stout, on the other hand the left posterior leaflet is thin and long
- It’s inseparably fused with the fibrous pericardium
- It’s found nearer to the sternum than to the vertebral column
Surfaces and Relationships
The superior surface of diaphragm projects on each side as dome or cupola into the thoracic cavity. Depressed area between the 2 domes is termed central tendon. The superior surface is covered by endothoracic fascia and is associated with the foundations of left and right pleura on the sides and to the fibrous pericardium in the middle.
The inferior surface of diaphragm is lined by the diaphragmatic fascia and parietal peritoneum.
- On the right side it’s related to (a) right lobe of the liver, (b) right kidney, and (c) right suprarenal gland.
- On the left side it’s related to (a) left lobe of the liver, (b) fundus of stomach, (c) spleen, (d) left kidney, and (e) left suprarenal gland.
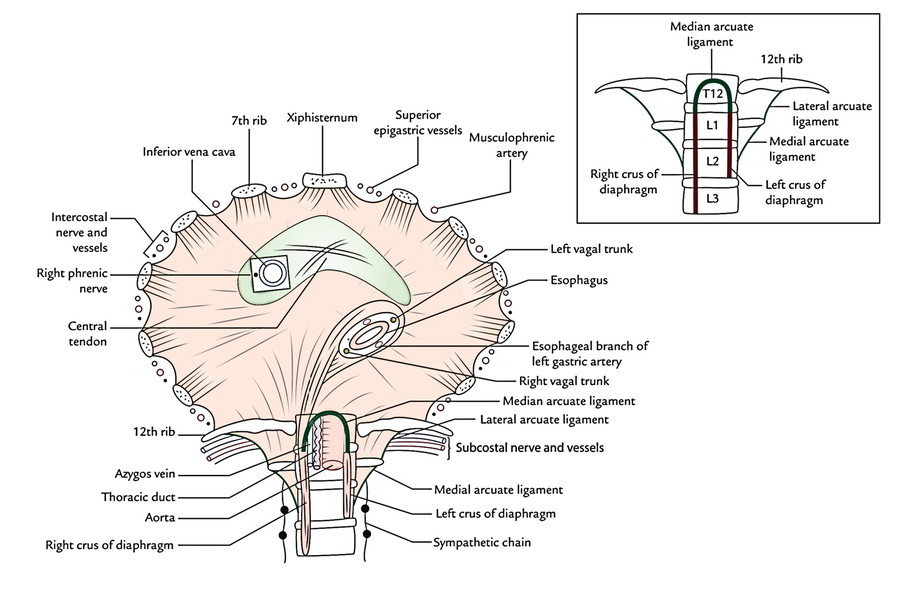
Openings of the Diaphragm
The openings of diaphragm are classified into 2 types: (a) major openings and (b) minor openings.
Major Openings
There are 3 referred to as major openings, viz.
- Vena caval opening
- Esophageal opening
- Aortic opening
Location, shape, and vertebral level of 3 major openings of the diaphragm.
| Opening | Location | Shape | Vertebral level |
|---|---|---|---|
| Vena caval opening | In the central tendon slightly to the right of median plane between the central and right posterior leaflets | Quadrangular or square | T8 (body) |
| Esophageal opening | Slightly to the left of median plane (The fibres of right crus split around the opening and act like pinch cock) | Oval or elliptical | T10 (body) |
| Aortic opening | In the midline behind the median arcuate ligament | Circular or round | T12 (lower border of the body) |
Structures going through 3 major openings of the diaphragm.
Opening | Structures passing through |
|---|---|
| Vena caval opening | 1. Inferior vena cava |
| 2. Right phrenic nerve | |
| Esophageal opening | 1. Esophagus |
| 2.Right and left vagal trunks | |
| 3. Esophageal branches of left gastric artery | |
| Aortic opening | From right to left these are: |
| 1. Azygos vein | |
| 2. Thoracic | |
| 3. Duct Aorta |
Key points to note.
- Contraction of diaphragm enlarges the caval opening to improve venous return.
- Contraction of diaphragm has a sphincteric effect on the esophageal opening (emergency-cock effect).
- Contraction of diaphragm has no effect on the aortic opening because only it’s outside the diaphragm.
Minor Openings
All these are unnamed. Structures going through these openings are as follows:
- Superior epigastric vessels go through the gap (space of Larry) between the muscular cases appearing from xiphoid process and 7th costal cartilage.
- Musculophrenic artery goes through the gap between the slides of origin from 7th to 8th ribs.
- Lower 5 intercostal nerves and vessels (i.e., 7th-l 1th) go through gaps between the adjoining costal skids.
- Subcostal nerves and vessels pass deep to the lateral arcuate ligament.
- Sympathetic chain enters deep to the medial arcuate ligament.
- Greater, lesser, and least splanchnic nerves pass by piercing the crus of diaphragm on the corresponding side.
- Hemiazygos vein pierces the left crus of the diaphragm.
Nerve Supply
The diaphragm is supplied by:
- Left and right phrenic nerves, and.
- Lower 5 intercostal and subcostal nerves.
The phrenic nerves are both motor and sensory. The right phrenic nerve gives motor innervation to the right half of the diaphragm up to the right margin of esophageal opening, and left phrenic nerve gives motor innervation to the left half of the diaphragm up to the left margin of the esophageal opening.
The phrenic nerves supply sensory innervation to the central tendon of the diaphragm, and pleura and peritoneum related to it.
The intercostal supply the peripheral parts of the diaphragm.
Arterial Supply
The diaphragm is supplied by the following arteries:
- Superior phrenic arteries (also named phrenic arteries) from thoracic aorta.
- Inferior phrenic arteries, from the abdominal aorta.
- Pericardiophrenic arteries, from the internal thoracic arteries.Musculophrenic arteries, the terminal branches of the internal thoracic arteries.
- Superior epigastric arteries, the terminal branches of the internal thoracic arteries.
- Lower 5 intercostal and subcostal arteries from the aorta.
Lymphatic Drainage
The lymph from diaphragm is drained into these groups of lymph nodes:
- Anterior diaphragmatic lymph nodes, situated behind the xiphoid process.
- Posterior diaphragmatic lymph nodes, situated near the aortic orifice.
- Right lateral diaphragmatic nodes, situated near the caval opening.
- Left lateral diaphragmatic nodes, situated near the esophageal opening.
Activities Of Diaphragm
The diaphragm acts to subserve these functions:
1. Muscle of inspiration: The diaphragm is the chief/ primary muscle of respiration. When it contracts, it descends and raises the vertical diameter of the thoracic cavity.
2. Muscle of abdominal staining: The contraction of diaphragm alongside contraction of muscles of anterior abdominal wall increases the intra-abdominal pressure to evacuate the pelvic contents (voluntary expulsive efforts, example, micturition, defecation, vomiting, and parturition).
3. Muscle of weight lifting: By taking deep breath and closing the glottis, if possible to raise the intra ¬ abdominal pressure to this kind of extent that it’ll help support the vertebral column and prevent its flexion. This helps the postvertebral muscles in lifting the colossi.
4. Thoraco-muscular heart: The descent of diaphragm reduces the intrathoracic pressure and at the exact same time raises the intra-abdominal pressure. This pressure change compresses the inferior vena cava, and therefore its blood is pushed upward into the right atrium.
5. Sphincter of esophagus: The fibres of the right crus of diaphragm subserve a sphincteric control over the esophageal opening.
Clinical Significance
1. Diaphragmatic paralysis (paralysis of diaphragm): The unilateral damage of phrenic nerve results in unilateral diaphragmatic paralysis. The illness is diagnosed during fluoroscopy when an elevated hemidiaphragm is observed on the side of lesion, and revealing paradoxical movements. The bilateral damage of phrenic nerves results in finish diaphragmatic paralysis. It’s a serious illness as it might cause respiratory failure.
2. Hiccups: They happen because of involuntary spasmodic contractions of the diaphragm escorted by the closing of the glottis. Hiccups normally happen after eating or drinking as a consequence of gastric irritation.
The pathological factors behind hiccups contain diaphragmatic irritation, phrenic nerve irritation, craze, and uremia.
Development
The diaphragm grows in the region of neck from the subsequent 4 structures:
- Septum transversum, ventrally
- Pleuroperitoneal membranes at the sides
- Dorsal mesentery of esophagus, dorsally
- Body wall, peripherally
Most likely
- Central tendon of diaphragm grows from septum transversum.
- Domes of diaphragm grow from pleuroperitoneal membrane.
- Part of diaphragm around the esophagus develops from the dorsal mesentery of esophagus.
- Peripheral part of diaphragm, grows from the body wall.
The musculature of diaphragm develops from 3rd, 4th, and 5th cervical myotomes (C3, C4, C5), for this reason it gets its motor innervations from C3, C4, and C5 spinal sections (i.e., phrenic nerve). Afterwards, when diaphragm descends from the neck to its certain position (i.e., thoraco-abdominal junction), its nerve supply is dragged down. This clarifies the long course of the phrenic nerve.
Clinical Significance
Diaphragmatic Hernias
Congenital
The different types of congenital diaphragmatic hernias regions follows:
- Posterolateral hernia (commonest congenital diaphragmatic hernia: In this illness, there’s herniation of abdominal contents into the thoracic cavity, which compress the lung and heart. The herniation takes place via the gap (pleuroperitoneal hiatus) between the costal and vertebral sources of the diaphragm referred to as foramen of Bochdalek. The gap stays because of failure of closing of pleuroperitoneal canal. It takes place usually on the left side.
- Retrosternal hernia: It happens via the gap between the muscular skids of origin from xiphisternum and 7th costal cartilage (space of Larry or foramen of Morgagni). It’s much more common on the right side. So hernial sac generally is located between pericardium and right pleura. Generally it causes no symptoms in the babies, but in afterwards age, the patients complain of suffering and dysphagia (difficulty in swallowing).
- Paraesophageal hernia: In this state, there’s defect in the diaphragm to the right and anterior to the esophageal opening. The anterior wall of the stomachrolls upwards in the hernial sac via this defect, until it becomes upside down in the thoracic cavity. An essential attribute of paraesophageal hernia is the fact that the normal relationship of gastroesophageal junction in regard to diaphragm isn’t touched.
Acqiured
The acquired diaphragmatic hernias could be either traumaticor hiatal (skidding).
- Traumatic hernia: It may take place because of an open injury to the diaphragm by the penetrating wounds or closed injury to the diaphragm in road traffic injuries resulting in unexpected serious rise in the intra-abdominal pressure.
- Hiatal (slipping) hernia: This is the commonest of all the internal hernias. In slipping hernia, the gastroesophageal junction and cardiac end of stomach slips up in the thoracic cavity, however only anterolateral portion of the herniated stomach is covered by peritoneum, for that reason the stomach itself isn’t inside the hernial sac. The hiatal hernia is caused by the weakness of the diaphragmatic muscle enclosing the esophageal opening and increased intra-abdominal pressure. This can cause regurgitation of acid contents of stomach into the esophagus resulting in peptic esophagitis. The patient complains of heart burn. The sliding hernia is generally related to short esophagus.

 (60 votes, average: 4.88 out of 5)
(60 votes, average: 4.88 out of 5)