The Collar bone or Clavicle (L. clavicle = key) is the long bone, having a slight S-shaped curve. Horizontally collar bone lies at the junction of root of the neck and trunk on the frontal aspects of body. Collar bone articulates along with the sternum and 1st rib cartilage and also vertically with the acromion process of the scapula. It can be palpated through its entire extent as it is subcutaneous and acts the only bony attachment between the trunk and upper limb.
Functions
The functions of the clavicle are below:
- It serves as a strut for keeping the upper limb far from the trunk to ensure that it can move freely. This enables free swing of the upper limb for several prehensile acts like holding, catching, etc.
- It transmits forces from the upper limb to the axial skeleton (sternum).
- It provides an area for the attachment of muscles.
Peculiarities
The peculiar features of the clavicle are as follows:
- It is the only long bone which lies horizontally.
- It has absolutely no medullary cavity.
- It is subcutaneous throughout its extent.
- It is the 1st bone to start ossifying (somewhere between the fifth and sixth week of intrauterine life) and very last bone to finish its ossification (at 25 years).
- It is the only long bone which ossifies by two primary centers.
- It is the only long bone which ossifies in membrane other than its medial end (cf. long bones ossify in cartilage).
-
It might be pierced inside out by cutaneous nerve (intermediate supraclavicular nerve).
Parts
The clavicle is composed of three parts: two ends (medial and lateral) and a shaft:
Ends
- The lateral (acromial) end is flattened above downwards and also articulates with medial margin of the acromion process.
-
The medial (sternal) end is enlarged and quadrilateral. It articulates with the clavicular notch of the manubrium sterni.
Shaft
The shaft is curved. Its medial two-third is round and convex forwards, plus its lateral one-third is flattened and concave forwards. The inferior surface of the shaft has a small longitudinal groove in its own middle third.
Anatomical Position and Side Determination
The side of clavicle can be identified by holding the bone horizontally as though its flattened end lies on the lateral side and its enlarged quadrilateral end lies on the medial side. The convexity of its medial two-third and concavity of its lateral one-third face forwards having longitudinal groove in the middle third of shaft facing inferiorly.Features and Attachments
Lateral End/Acromial End
It is flattened above downwards. An oval facet on this end articulates using the facet on the medial margin of the acromion to form acromioclavicular joint. The lateral end provides connection to fibrous capsule of acromioclavicular joint.
Medial End/Sternal End
The enlarged medial end has a saddle-shaped articular surface, that articulates using the clavicular notch of manubrium sterni to develop sternoclavicular joint. It provides connection to:
- Fibrous capsule
- Articular disc
- Interclavicular ligament.
Shaft
The shaft of the clavicle is split into two parts: lateral one-third and medial two-third. The medial two-third of shaft is convex forward but lateral one-third is concave forward.
Lateral One-third It is flattened from above downwards. It has two surfaces, i.e., superior and inferior, and two borders, i.e., anterior and posterior.
Surfaces
Superior surface: It is subcutaneous somewhere between the attachments of deltoid and trapezius.
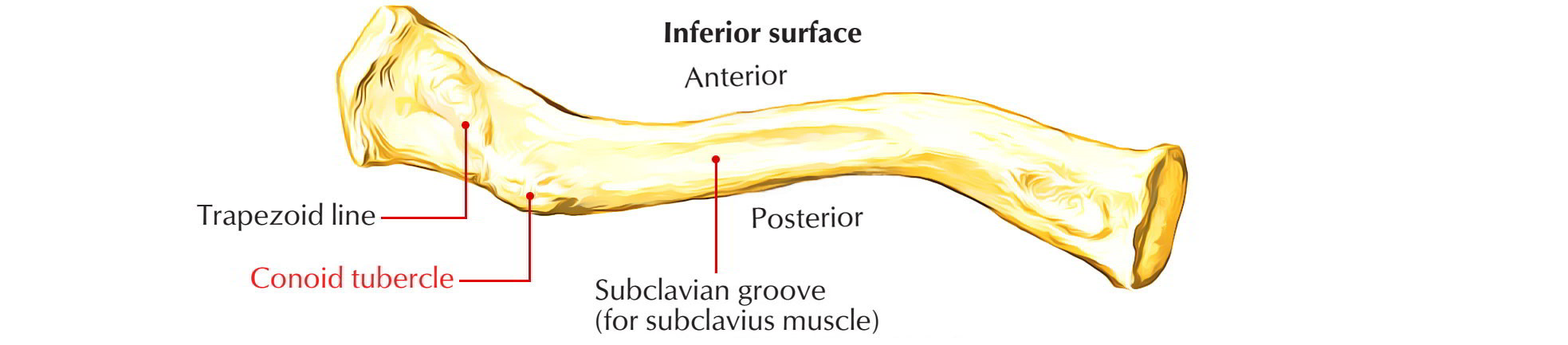
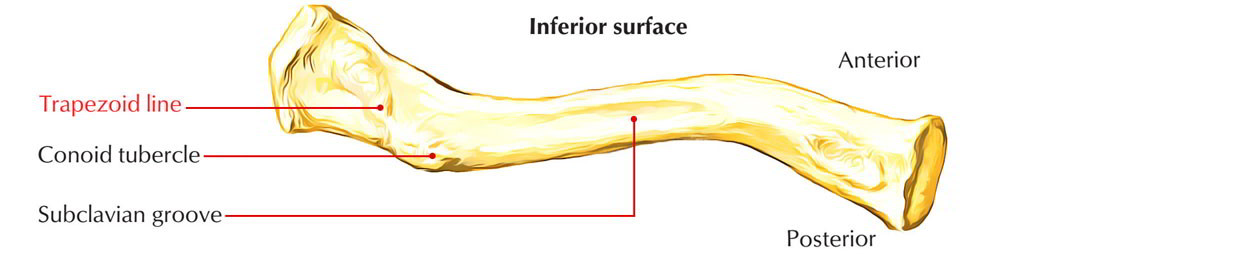
Inferior surface: It provides a conoid tubercle and trapezoid ridge, which provide attachments to conoid and trapezoid component of coracoclavicular ligament, respectively.
The conoid tubercle lies on the inferior surface close to the posterior border at the junction of the lateral one-fourth and medial three-fourth of the clavicle. The trapezoid ridge extends forwards and also laterally from conoid tubercle.
Borders
Anterior border: It is concave forwards and provides origin to deltoid muscle. A small tubercle know as deltoid tubercle might exist on this border.
Posterior border: It is convex backwards and supplies insertion to the trapezius muscle.
Medial Two-third It is cylindrical in shape and provides four surfaces: anterior, posterior, superior, and inferior.
Anterior surface: It is convex forwards and provides origin to clavicular head of pectoralis major.
Posterior surface: It is concave backwards and provides origin to sternohyoid muscle close to its medial end. The lateral component of this surface forms the anterior boundary of cervico-axillary canal and relates to the following structures:
- Trunks of brachial plexus.
-
Third part of subclavian artery.
Superior surface: The clavicular head of sternocleidomastoid muscle originates from medial half of this surface.
Inferior surface: It provides the following features:
- Costoclavicular ligament is attached to an oval impression at its medial end.
- Subclavius muscle is inserted into the subclavian groove on this surface.
- Clavipectoral fascia is attached to the margins of subclavian groove.
-
Nutrient foramen of clavicle is found on the lateral end of the subclavian groove.
Muscles and Ligaments Connected to the Clavicle
| Muscles | Ligaments |
|---|---|
| Pectoralis major | Coracoclavicular |
| Sternocleidomastoid (clavicular head) | Costoclavicular |
| Deltoid | Interclavicular |
| Trapezius | - |
| Subclavius | - |
Ossification
Subclavius Ossification
The ossification of clavicle is membranocartilaginous. Whole of it ossifies in the membrane with the exception of its medial end which ossifies in the cartilage. The clavicle begins to ossify before some other bone in the body.
It ossifies by four ossification centres- two primary centres for shaft and two secondary centres, one for each end.
Ossification centers of the Clavicle
| Site of appearance | Time of appearance | Time of fusion | ||
|---|---|---|---|---|
| Two primary centres (medial and lateral) in the shaft. | 5-6 weeks of intrauterine life (IUL). | 45th day of IUL. | ||
| Secondary centre at sternal end | 19-20 years (2 years earlier in female) | 25th year | ||
| Secondary centre at the acromial end (occasional) | 20th year | Fuses immediately. | ||
Clinical Relevance
Fracture of Clavicle
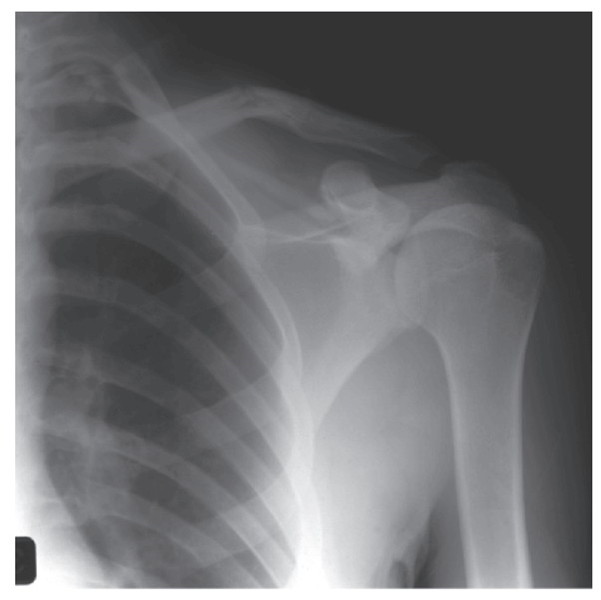
Fracture of clavicle he clavicle is the most commonly fractured bone in the body. It commonly fractures at the junction of its lateral one-third and medial two-third due to blows to the shoulder or indirect forces, usually as a result of strong impact on the hand or shoulder, when person falls on the outstretched hand or the shoulder. When fracture occurs, the lateral fragment is displaced downward by the weight of the upper limb because trapezius alone is unable to support the weight of the upper limb. In addition, the lateral fragment is drawn medially by shoulder adductors viz. teres major, etc. The medial fragment is slightly elevated by the sternocleidomastoid muscle. The characteristic clinical picture of the patient with fractured clavicle is that of a man/woman supporting his sagging upper limb with the opposite hand. The fracture at the junction of lateral one- third and medial two-third occurs because:
- This is the weakest site.
- Two curvatures of clavicle meet at this site.
-
The transmission of forces (due to impact) from the clavicle to scapula occur at this site through coracoclavicular ligament.
Congenital Anomalies
- Clavicular dysostosis: It is a clinical condition in which medial and lateral component of clavicle remain separate as a result of nonunion of two primary centers of ossification.
-
Cleidocranial dysostosis: It is a clinical condition characterized by partial or complete absence of clavicle associated with defective ossification of the skull bones.
The clavicle is absent in animals where the upper limbs are used only for walking and weight transmission, and except grasping such as horse, etc.
One of the two primary centers of clavicle is regarded as precoracoid element of reptilian shoulder girdle.
Growing end of clavicle: The sternal end of clavicle is its growing end, because epiphysis at this end appears at the age of 19-20 years and unites with the shaft at the age of 25 years. It is the last of all the epiphyses in the body to fuse with the shaft. The radiological appearance of this particular epiphysis in females validates their bone age for legal consent to marriage.

 (59 votes, average: 4.61 out of 5)
(59 votes, average: 4.61 out of 5)