Prostate is a fibromuscular glandular organ encompassing the prostatic urethra. It is pyramidal-shaped. The various secretions of the prostate gland comprise of acid phosphatase, fibrinolysin, citric acid, amylase, prostate-specific antigen (PSA), and prostaglandins. Most of the seminal fluid is created by its secretions. The female homologue of prostatic urethra is paraurethral glands (of Skene).
Location
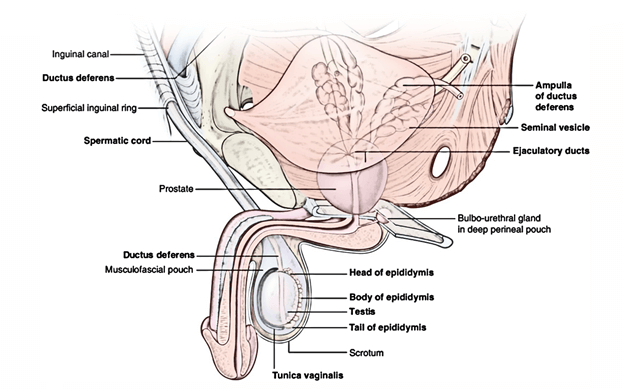
The location of the prostate is in the lower pelvis below the neck of the urinary bladder and above the urogenital diaphragm. It is situated behind the lower part of the pubic symphysis and in front of the rectal ampulla. It’s covered on every side by the levator ani muscle.
Shape, Size, and Measurements
The prostate is similar to an inverted cone in shape and resembles a chestnut in look. It presents these measurements:
- Weight: 3 g.
- Width (at base): 4 cm.
- Length: 3 cm.
- Thickness: 2 cm.
The prostate belongs to the group of organs which have more width than length, like caecum, coeliac trunk, etc.
External Features and Relations
The prostate presents the following external features:
- Apex.
- Base.
- 4 surfaces (anterior, posterior and 2 inferolateral).
Apex
It’s pointed downward and rests on the superior surface of the urogenital diaphragm.
Base
It’s pointed upward and encircles the neck of the urinary bladder with which it’s constant structurally. The junction is marked by a circular groove. The base is pierced by the urethra in the median plane in the junction of its anterior one-third and posterior two-third.
Surfaces
- Anterior surface: It’s narrow and convex from side to side. It’s situated 2 cm supporting the pubis symphysis. It’s divided from the symphysis by the retropubic space (of Retzius) filled up with extraperitoneal fat. A little above the apex, this surface is pierced by the urethra.
- Posterior surface: It’s broad and flat and is located in front of the ampulla of the rectum, from which it’s divided by the fascia of Denonvilliers. The posterior surface is split into small upper and bigger lower regions by a transverse sulcus, that is pierced on every side of the median plane by the ejaculatory duct. The upper regions represent the median lobe and the lower area is split by a median sulcus into 2 lateral lobes.
- Inferolateral surfaces: All these are linked to the anterior fibres of levator ani (levator prostate).
Lobes of The Prostate
The prostate is split into 5 lobes:
- Anterior lobe (isthmus).
- Posterior lobe.
- Median lobe.
- 2 lateral lobes.
Anterior Lobe
The anterior lobe is located in front of the urethra and attaches both lateral lobes. It’s devoid of the glandular tissue and regularly named isthmus.
Posterior Lobe
The posterior lobe is located behind the ejaculatory ducts and median lobe and attaches both lateral lobes. The primary carcinoma of the prostate starts in this lobe.
Median Lobe (Middle Lobe)
The median lobe is wedge shaped and is located behind the upper part of the urethra and in front of ejaculatory ducts. Its base generates an elevation in the apex of trigonum vesicae referred to as uvula vesicae. The median lobe normally projects into the prostatic urethra lifting a ridge referred to as urethral crest.
It includes much of the glandular tissue and is a familiar site of adenoma.
Lateral Lobes
The lateral lobes are located 1 on every side of the urethra. On the posterior outermost layer of the prostate, 2 lateral lobes are divided from every other by posterior median sulcus. The lateral lobes include some glandular tissue and for that reason adenoma may originate here in the old age.
Structures inside The Prostate
All these are as follows:
- Prostatic urethra traverses vertically downward via the gland in the junction of its anterior one-third and posterior two-third and opens on the anterior surface just above the apex.
- Ejaculatory ducts traverse the gland posterolateral to the median lobe and open in the urethra.
- Prostatic utricle is a mucous cul de sac about 6 mm long which goes upward and backwards from the prostatic urethra, behind the median lobe.
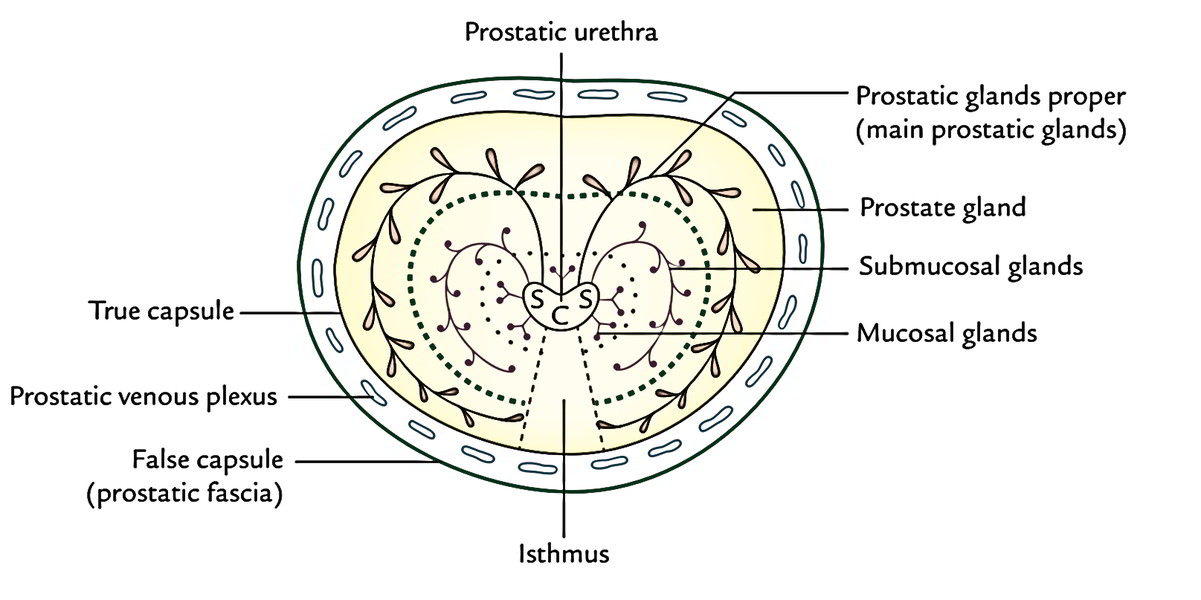
Capsules of The Prostate
The prostatic capsules are 2 in number in normal gland and 3 in number if gland is influenced by benign hypertrophy of the prostate.
- True capsule: It’s created by the condensation of peripheral fibrous stroma of the gland, for this reason closely related to the gland.
- Fictitious capsule (prostatic sheath): It’s originated from the pelvic fascia. It’s outside the true capsule and envelops the prostate gland and urinary bladder in exactly the same compartment.
- Surgical/pathological capsule: When the adenoma of the gland enlarges, the peripheral part of the organ becomes compressed. This compressed part of the gland is named surgical or pathological capsule.
The prostatic venous plexus is located between the true and false capsules with the exception of on the posterior outermost layer of the gland.
(cf. the venous plexus of the thyroid gland is located deep to both true and fake capsules).
Supports of The Prostate
These are:
- Urogenital diaphragm: The apex of the gland rests on it and the prostatic sheath (bogus capsule) is constant with its superior fascia.
- Two pairs of puboprostatic ligaments: They go from the prostatic sheath (bogus capsule) to the rear of the pubic bones. The medial pair is located near the apex of the gland and the lateral pair close to the base.
- Rectovesical fascia of Denonvilliers: The posterior aspect of prostatic sheath sticks to this fascia posteriorly.
Fascia of Denonvilliers (rectovesical fascia): It’s a fascial septum between prostate and ampulla of the rectum and goes from the floor of rectovesical pouch to the perineal body. Origin of the fascia has a developmental basis. In foetus, the rectovesical pouch is deep and divides the prostate from the rectum. In afterwards life, 2 layers of the peritoneum between prostate and rectum fuse to create this fascia. The carcinoma prostate only seldom enters this fascial impediment so that engagement of the rectum is uncommon.
Structure of The Prostate
The prostate gland is created from fibrous tissue (1/4), muscular tissue (1/4), and glandular tissue (1/2). The glandular tissue is composed of tubuloalveolar glands arranged in 3 concentric groups (mucosal, submucosal, and chief); all of them open into the urethra. The fibro muscular tissue creates the stroma and the glandular tissue types the parenchyma of the prostate gland. The lumen of tubuloalveolar gland includes small colloid masses named corpora amylacea.
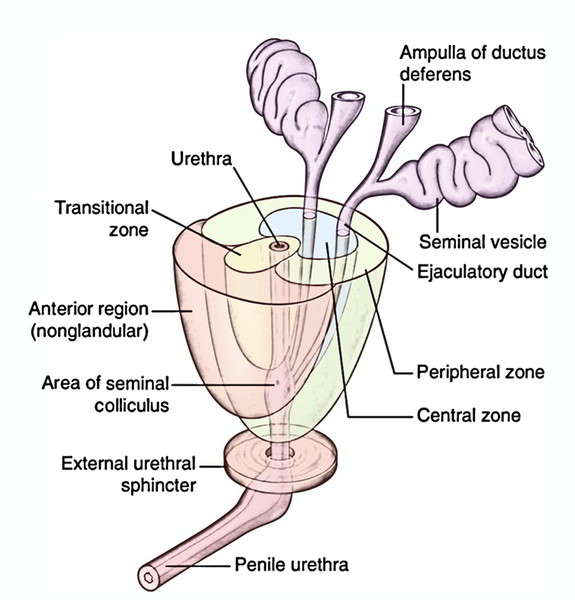
Structural Zones of The Prostate Gland
Histologically, the prostate gland will not reveal the lobular pattern as normally described in Gross Anatomy; instead there are 2 well defined concentric zones divided by an ill-defined atypical fibrous layer. The zones are absent anteriorly.
- Outer zone: The bigger outer zone consists of long branching glands (prostatic gland appropriate). The ducts of these glands arch backward and open in the prostatic sinus below the colliculus seminalis. This zone is the common site of carcinoma prostate.
- Inner zone: The smaller inner zone consists of outer submucosal glands, which open in the prostatic sinus in the level of colliculus seminalis. Deep to these glands are simple mucosal glands (suburethral glands), that are short and open all around the urethra above the level of colliculus seminalis.
All hypertrophies of the prostate originate from these mucosal (suburethral/subcervical) glands. For that reason, the inner zone of prostate is the common site of benign prostatic hypertrophy (BPH).
Arterial Supply
The prostate gland is supplied by the branches of inferior vesical, middle rectal, and internal pudendal arteries.
Venous Drainage
The veins from the prostate create a rich venous plexus around the sides and base of the gland and inhabit the space between the true and fictitious capsules. It gets the deep dorsal vein of the penis in front and is continuous above with the vesical venous plexus.
The style of venous drainage from the prostatic venous plexus follows 2 pathways:
- Into internal iliac veins via the posterior ligaments of the urinary bladder.
- Into internal and external vertebral venous plexus (of Batson) via veins going through anterior sacral foramina. The communication between the vesical and vertebral venous plexuses is valveless.
The venous drainage of the prostate follows 2 pathways:
- Prostatic venous plexus ^ internal iliac veins ^ IVC. This pathway clarifies the metastasis of cancer prostate into the heart and lungs.
- Prostatic venous plexus ^ vertebral venous plexus (of Batson) ^ intracranial dural venous sinuses. This pathway describes the metastasis of cancer prostate into the vertebral column and brain.
Lymphatic Drainage
The lymphatics from the prostate drain into the internal iliac, external iliac, and sacral groups of the lymph nodes.
Nerve Supply
The prostate is supplied by the following nerves:
- The sympathetic supply is supplied by the superior hypogastric plexus. The preganglionic sympathetic fibres originate from L1 and L2 spinal sections.
- The parasympathetic supply is offered by the pelvic splanchnic nerves which express preganglionic fibres from S2, S3, S4 spinal sections.
Development of The Prostate Gland
The prostate grows from these sources:
- The parenchyma (glandular portion) of the gland grows in the 3rd month of intrauterine life (IUL) as a series of endodermal buds (outgrowths) from the lining of archaic urethra and adjoining portion of the urogenital sinus.
- The stroma of the gland grows in the 4th month of IUL from the surrounding mesenchyme originated from the splanchnic layer of mesoderm.
Changes in The Prostate with age
The age-associated changes in prostate are as follows:
- In youth, the prostate gland is small and is composed primarily of fibromuscular stroma and rudiments of ducts.
- At puberty, there’s a surprising rise in the size of gland below the effect of male hormone (testosterone). It becomes twice of its prepubertal size. There’s fast proliferation of prostatic follicles which begin secretion.
- During the 3rd decade, there are atypical epithelial infoldings in the lumen of the follicles, making them atypical.
- During the fourth decade, the size of prostate stays continuous. The epithelial infoldings in the lumen slowly vanish and amyloid concretions (amyloid bodies) appear in the follicles.
- During the fifth decade (i.e., after 50 years of age), some measure of prostatic hypertrophy is always present. It’s as much an indication of aging as the graying of hair. In certain cases, the gland, nevertheless, is reduced in size referred to as senile atrophy.
Clinical Significance
Benign Prostatic Hypertrophy (BPH)
After 50 years old, the prostate gland is enlarged because of hypertrophy of median lobe (hypertrophy of subcervical glands of Albarran) creating an adenoma. The BPH generally includes the median lobe, which compresses the prostatic urethra and obstructs the pee flow. The enlargement of uvula vesicae because of enlarged median lobe effects in the formation of postprostatic pouch of stagnant urine in the urinary bladder behind the internal urethral orifice. Medically BPH presents as: (a) increased frequency of urination, (b) urgency of urination, (c) difficulty in starting and stopping urination, and (d) a sense of incomplete emptying of the urinary bladder.
The surgical removal of adenoma is known as prostatectomy. The adenoma is enucleated, leaving behind both the capsules and the prostatic venous plexus between them.
After prostatectomy, the patient becomes infertile since the mechanism of internal urethral sphincter is touched and semen enters into the urinary bladder during ejaculation.
There are several surgical tactics of prostatectomy, viz., suprapubic, retropubic, perineal, and transurethral.
Most adenomatous enlargements of the prostate are now resected transurethrally.
Prostatic Carcinoma
It generally takes place following the age of 50 years. The carcinoma is often seen in the outer (peripheral) zone which generally includes the posterior lobe. Medically, it presents as:
- Pain in perineum.
- Urinary obstruction.
- Trouble in urination.
For diagnosis, per rectal examination reveals unusual, hard, rigid prostate, and absence of median groove in its posterior surface. The serum levels of acid phosphatase and prostate specific antigen (PSA) are utilized in diagnosis and management of prostate cancer.
The metastasis of prostatic carcinoma typically appears in the lumbar vertebrae and pelvis.

 (61 votes, average: 4.48 out of 5)
(61 votes, average: 4.48 out of 5)