The hormones secreted by the thyroid gland contain triiodo-thyronine (T3), tetraiodothyronine (T4; generally termed thyroxine) and calcitonin. The thyroid gland is the largest endocrine gland of the body, which subserve these functions:
- Modulate the basal metabolic rate.
- Excite the psychosomatic development of the body.
- Play an essential function in calcium metabolism.
Special Fetures
The special features of the thyroid gland are:
- It’s the only endocrine gland that is situated superficially in the body, for this reason reachable for physical examination.
- It’s the only endocrine gland that depends on external environment for raw material, iodine, to synthesize its hormones.
- It’s the only endocrine gland, which doesn’t pour its hormones into blood immediately after formation but stores them and after that discharges them in blood to be used as and when needed.
- It’s one of the organs of the body having an extremely rich blood circulation.
Location
The thyroid gland lies in the lower part of the front and side of the neck reverse to the C5, C6, C7 and T1 vertebrae, clasping the upper part of the trachea.
Parts and Features
It’s H-shaped and being composed of vertical left and right lateral lobes and a horizontal isthmus attaching them across the midline. Occasionally a small pyramidal lobe projects upwards from the isthmus generally to the left of the midline. Not infrequently, it’s joined to the body of the hyoid bone by a fibrous or fibromuscular band named levator glandulae thyroideae.
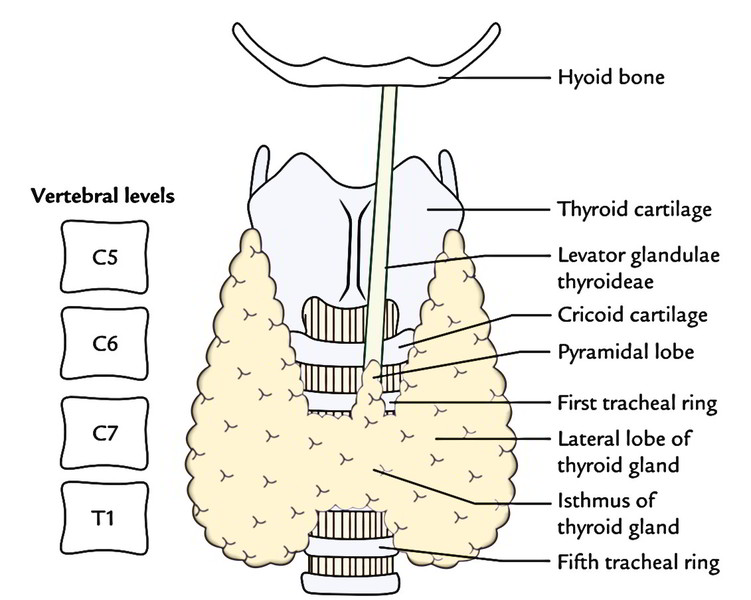
Every lateral lobe of the gland goes upwards to the oblique line of the thyroid cartilage and below up to the 5th or 6th tracheal ring.
The isthmus goes across the midline in front of the second, third and 4th tracheal rings.
Weight and Measurements
The thyroid gland weighs about 25 grams. Every lobe of the thyroid gland is 5 cm long, 3 cm wide and 2 cm thick (5 X 3 X 2 cm). The isthmus measures about 1.25 cm in both, vertical and transverse diameters.
The thyroid gland is generally bigger in females and increases even more in size during menstruation and pregnancy.
Capsule of The Thyroid Gland
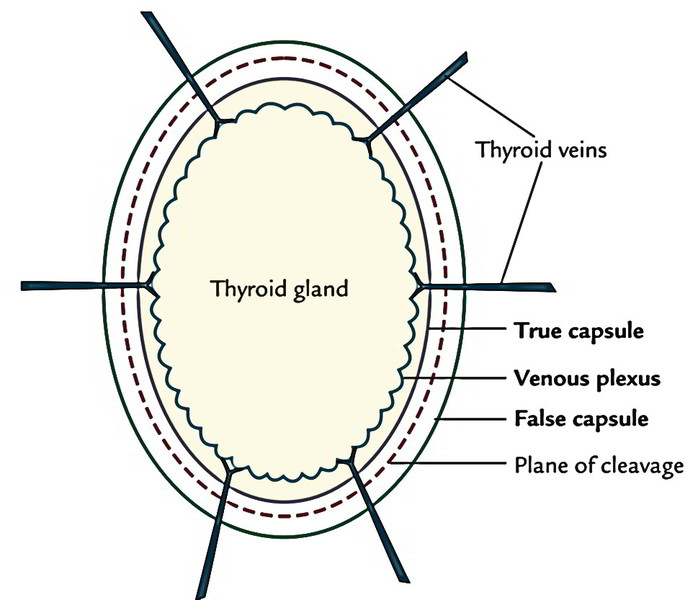
The thyroid gland is invested by 2 capsules: an inner true capsule and an outer bogus capsule.
True capsule: It’s created by the peripheral conholesation of the fibrous stroma of the gland
Fictitious capsule: It’s originated from the carving of the pretracheal fascia. The significant features of the fictitious capsule are:
- It’s thin along the posterior border of the lateral lobe.
- It’s thick on the medial surface of the lateral lobe.
- Delineated above, the pretracheal fascia after enclosing the thyroid gland is connected to the oblique lines of the thyroid cartilage and the body of the hyoid bone in the midline. On the medial surface of thyroid lobe it thickens to create the suspensory ligament ofBerry, which attaches the lobe to the cricoid cartilage.
- The holese venous plexus unlike that of the prostate gland is located deep to true capsule. Thus, to avert hemorrhage during thyroidectomy, the thyroid gland is removed together with the true capsule.
- In case of prostate gland, the venous plexus is located between its true and fictitious capsules and, for that reason, during surgical removal of prostate gland (prostatectomy) prostate gland is removed; leaving behind both the capsules.
Clinical Significance
Occasionally the thyroid tumor goes backwards, as the capsule is thin along the posterior edges of the lateral lobes, compressing the adjacent structures without creating a visible swelling on the very front of the neck.
The thyroid gland moves up and down during consuming because its capsule is connected to laryngeal cartilages and hyoid bone, which moves up and down during consuming. Hence thyroid swellings can be differentiated medically from other swellings in the region of the neck.
Relationships
Relationships of the Thyroid Lobe
Every lobe of the thyroid gland is about pyramidal (conical) and presents apex, base, 3 surfaces (lateral, medial and posterolateral) and 2 edges (anterior and posterior):
Apex: The apex is pointed upwards and somewhat laterally. It goes up to the oblique line of thyroid cartilage where it’s limited above by the connection of sternothyroid muscle. The apex is sandwiched between the inferior constrictor medially and sternothyroid laterally.
Base: The base goes up to the 5th or 6th tracheal ring. It’s related to inferior thyroid artery and recurrent laryngeal nerve.
Lateral (superficial) surfaces: It’s convex and is covered by:
- 3 strap muscles (sternothyroid, sternohyoid and superior belly of omohyoid) and
- anterior border of sternocleidomastoid overlapping it inferiorly
Medial surface is related to:
- 2 tubes: trachea and esophagus
- 2 muscles: inferior constrictor and cricothyroid and
- 2 cartilages: cricoid and thyroid
Posterolateral surface is related to carotid sheath and its contents (common carotid artery, internal jugular vein and vagus nerve). The ansa-cervicalis is embedded in the anterior wall of the sheath while cervical sympathetic chain is located posterior to sheath in front of prevertebral fascia.
Anterior border is thin and splits superficial and medial surfaces. It’s related to anterior branch of the superior thyroid artery.
Posterior border is thick and rounded. It splits the medial and the posterior surfaces. It’s related to:
- longitudinal arterial anastomosis between superior and inferior thyroid arteries and
- parathyroid glands
Relationships of Isthmus
The isthmus is horizontal and presents 2 surfaces- anterior and posterior and 2 edges- superior and inferior.
Anterior surface is related to:
- strap muscles (sternohyoid and sternothyroid) and
- anterior jugular veins
Posterior surface is related to second, third and 4th tracheal rings.
Superior border is associated with anastomosis between the anterior branches of 2 superior thyroid arteries.
Inferior border: Along this border inferior thyroid vein issue and thyroidea ima artery (when present) enters.
Arterial Supply
The gland is extremely vascular and is supplied by the following arteries:
Superior Thyroid Artery
It’s a branch of the external carotid artery. It runs downwards and forwards in business with the external laryngeal nerve, which it makes near the upper pole of the thyroid lobe. At the apex of the lobe, it splits into anterior and posterior branches. The anterior branch first descends along the anterior border of the lobe and after that proceeds along the upper border of the isthmus to anastomose with its chaps of opposite side. The posterior branch descends along the posterior border of the lobe to anastomose with the ascending branch of the inferior thyroid artery.
Superior thyroid artery supplies the upper one-third of the lobe and upper half of the isthmus.
Inferior Thyroid Artery
It’s a branch of thyrocervical trunk from the initial part of the subclavian artery. It first runs upwards along the medial border of scalenus anterior and after that enters medially behind the carotid sheath to get to the rear of the thyroid lobe, where it’s closely associated with the recurrent laryngeal nerve. The recurrent laryngeal nerve presents a varying relationship together with the artery. It might pass behind or in front of the loop of the artery or between the branches of the artery. The artery supplies four or five branches. 1 ascending branch anastomoses with the posterior branch of the superior thyroid artery.
The inferior thyroid artery supplies lower ⅔rd of the lobe and lower half of the isthmus.
Thyroidea Ima Artery (In 30% Cases)
It’s a branch of the brachiocephalic trunk or may originate directly from the arch of aorta. It enters the isthmus from below.
Accessory Thyroid Arteries
They originate from tracheal and esophageal arteries.
Venous Drainage
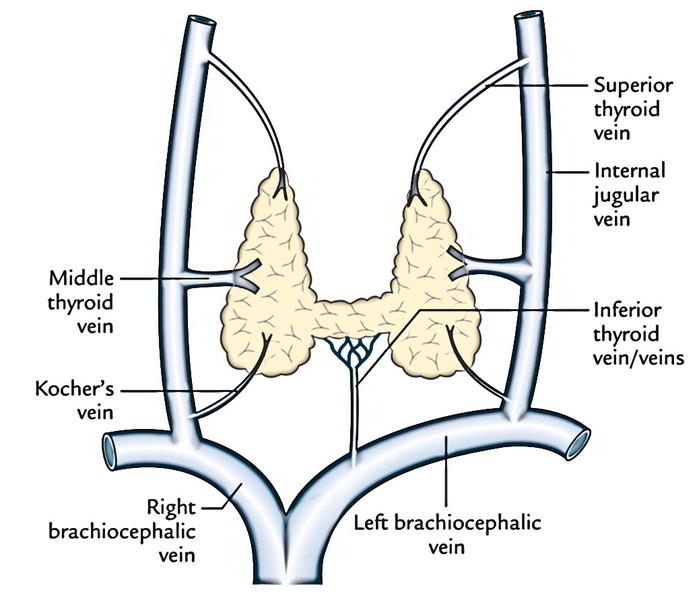
The venous blood from the thyroid gland is emptied by threeset of veins viz.
Superior thyroid vein: It comes at the upper pole of the thyroid lobe, runs upwards and laterally and empties into the internal jugular vein.
Middle thyroid vein: This short, wide venous channel issues at the middle of the lobe to shortly go into the internal jugular vein.
Inferior thyroid vein/veins: They come at the lower border of the isthmus, create plexus in front of the trachea and after that run downwards to drain into the left brachiocephalic vein.
Occasionally a fourth vein, the thyroid vein (of Kocher) comes between the middle and inferior thyroid veins to drain into the internal jugular vein.
Lymphatic Drainage
The lymph vessels emptying the thyroid gland are ordered intotwo groups, upper and lower and they follow the arteries:
The upper group empties in the prelaryngeal (being located in front of the larynx) and upper deep cervical (jugulo digastric) lymph nodes.
The lower group drains into pretracheal and lower deep cervical lymph nodes and group of lymph nodes along the recurrent laryngeal nerves. Those from lower part of isthmus drain into retrosternal or brachiocephalic nodes being located in the superior mediastinum.
The upper lymphatics follow superior thyroid artery andlower lymphatics follow the inferior thyroid arteries.
Nerve Supply
The thyroid gland is supplied by both sympathetic andparasympathetic nerve fibres:
- The parasympathetic supply is originated from the vagus and recurrent laryngeal nerves
- The sympathetic supply is originated from the superior, middle and inferior cervical sympathetic ganglia, but primarily from the middle one.
Microscopic Structure
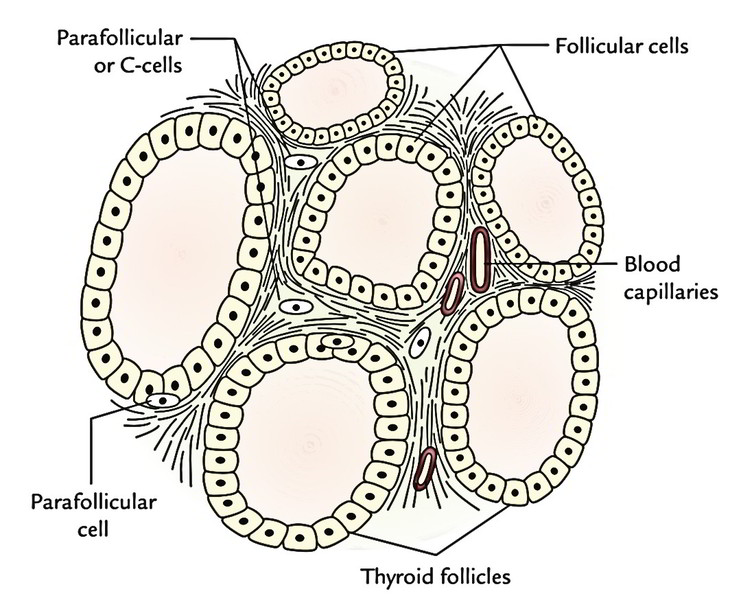
The thyroid gland contains 2 types of secretory cells: follicular and parafollicular.
The follicular cells are cuboidal epithelial cells creating the wall of spherical thyroid follicles. They secrete 2 hormones: thyroxine and triiodothyronine.
These hormones are necessary for normal growth and development, especially of the skeletal and nervous system.
The parafollicular cells or C cells are located primarily between the basement membrane and the follicular cells. A number of them also are located in the spaces between the follicles. They secrete a hormone named thyrocalcitonin (also termed calcitonin). It plays a significant function in calcium metabolism. It reduces the blood calcium level by lessening the reabsorption of the calcium by the renal tubules. Its effects are contrary to that of parathormone.
Clinical Significance
Goitre
Any enlargement of the thyroid gland with the exception of that during menstruation and lactation is named goitre. It might be connected with hypofunction or hyperfunction of the gland
Hypothyroidism takes place when there’s inadequate secretion of the T3 and T4. The reduced levels of T3 and T4 cause increased secretion of TSH.
Hypothyroidism causes cretinism in kids and myxedema in adults.
Hyperthyroidism (or thyrotoxicosis) takes place because of excessive secretion of T3 and T4. The thyrotoxicosis medically shows as: tachycardia, tremors and systolic bruit. The main effects are because of increased BMR.
Simple Goitre/Puberty Goiter
It’s an enlargement of the thyroid gland without signs of hyperthyroidism. It happens because of lack of iodine in diet. Remember iodine is crucial for synthesis of thyroid hormone. The reduced levels of T3 and T4 result in increased secretion of TSH from the pituitary gland The TSH causes hyperplasia of the thyroid gland Simple goitre usually happens in females at the age of puberty, thus it’s also referred to as puberty goitre.
Effects of Huge Enlargement of Thyroid Gland
The thyroid gland can enlarge backwards or downwards but it can not enlarge upwards as a result of connection of its fascial sheath and sternothyroid muscle to the thyroid cartilage.
The backward enlargement is common since the thyroid capsule is comparatively thin posteriorly. In backward enlargement, the gland immerses itself around the sides of trachea and esophagus.
This results in 3 characteristic pressure symptoms, viz.
- Dyspnea (difficulty in breathing), as a result of pressure on trachea.
- Dysphagia (trouble in swallowing), as a result of pressure on esophagus.
- Dysphonia (hoarseness of voice), because of pressure on the recurrent laryngeal nerve, which is located in the tracheoesophageal groove.
Mnemonic = 3D.
The downward growth supporting the sternum is termed retrosternal goitre. It can compress trachea resulting in dangerous dyspnea.
It can also cause acute venous compaction resulting in venous congestion.
Ligation of Thyroid Arteries during Thyroidectomy
Thesuperior thyroid artery and the external laryngeal nerve diverge from every other near the apex, the artery is located superficial and the nerve is located deep to the apex. For that reason, during thyroidectomy, the superior thyroid artery ought to be ligated as close to the apex of thyroid lobe as possible to prevent injury to the external laryngeal nerve.
The recurrent laryngeal nerve is located quite close to the inferior thyroid artery near the base of the thyroid lobe. For that reason, during thyroidectomy, the inferior thyroid artery ought to be ligated as far from the base of the thyroid lobe as possible to prevent injury to the recurrent laryngeal nerve.
Benign Tumors
Benign tumors may compress or also displace the contiguous structures on the other hand malignant growth tends to invade surrounding structures.
Development
The thyroid gland starts to grow as endodermal thickening in the midline of the floor of the pharynx instantly behind the tuberculum impar during third week of intrauterine life. This thickening is shortly depressed below the surface to create a diverticulum termed thyroglossal duct. This duct grows downwards across the tongue then descends in front of the neck. In the neck, it enters in front of hyoid bone, binds around its lower border to become retrohyoid and ultimately descends below the hyoid with little inclination to 1 side, generally to left to reach its unequivocal position (by the end of the 7th week) where its tip bifurcates and proliferates to create the bilateral terminal swellings, which enlarge to create the thyroid gland A portion of the duct near its tip occasionally forms the pyramidal lobe. The rest of the duct vanishes. The site of origin of thyroglossal duct is, nevertheless, marked by foramen caecum in the junction of the anterior ⅔rd and posterior ⅓rd of the tongue in adults. The thyroid is the first glandular tissue to grow and becomes functional during the third month.
The ultimobranchial bodies from 5th pharyngeal pouches and neural crest cells become integrated secondarily into thyroid gland and create parafollicular cells or C cells.
Clinical Significance
Congenital Anomalies
The development of the thyroid gland may account for the subsequent common congenital anomalies:
Thyroglossal cyst/fistula: Thyroglossal duct may continue and result in formation of thyroglossal cyst and fistula.
Ectopic thyroid: The Thyroid gland (thyroid tissue) may be seen at an abnormal position anywhere along the course of thyroglossal duct
- at the base of the tongue (lingual thyroid). In lingual thyroid, the mass of thyroid tissue is situated inside the tongue just below the foramen caecum and if large, it can cause trouble in swallowing by the baby
- above, behind or below the hyoid bone (suprahyoid, retrohyoid, or infrahyoid thyroid)
- 1 of the lobes might be absent
- Isthmus may be absent
- Descent of the thyroglossal duct may go past the certain position in the neck to superior mediastinum (retrosternal thyroid)
- Thyroid tissue might be situated far from the normal course of the thyroglossal duct, viz. in relation to carotid sheath, in the mediastinum, in the pericardium (aberrant thyroid).

 (63 votes, average: 4.54 out of 5)
(63 votes, average: 4.54 out of 5)