Synonym: Latin uterus; Greek hystera: womb; (viz., use of terms like hysterectomy).
Uterus is known as the child-bearing organ in females. The most important work of the uterus is to provide suitable site and environment for implantation of a fertilized ovum and development of the embryo.
- It’s a hollow thick-walled, muscular organ with a narrow lumen.
- It’s situated obliquely in the lesser pelvis between urinary bladder and rectum.
- Its long axis is horizontal if the bladder is empty in the erect position.
- Superiorly, on every side, it interacts with all the uterine tube and inferiorly with the vagina.
Shape and Size
It’s pear shaped, being flattened anteroposteriorly.
Measurements.
- Length: 3 inches (7.5 cm).
- Width (at fundus): 2 inches (5 cm).
- Thickness: 1 inch (2.5 cm).
- Weight. 30-40 grams.
Subdivisions/Parts of The Uterus
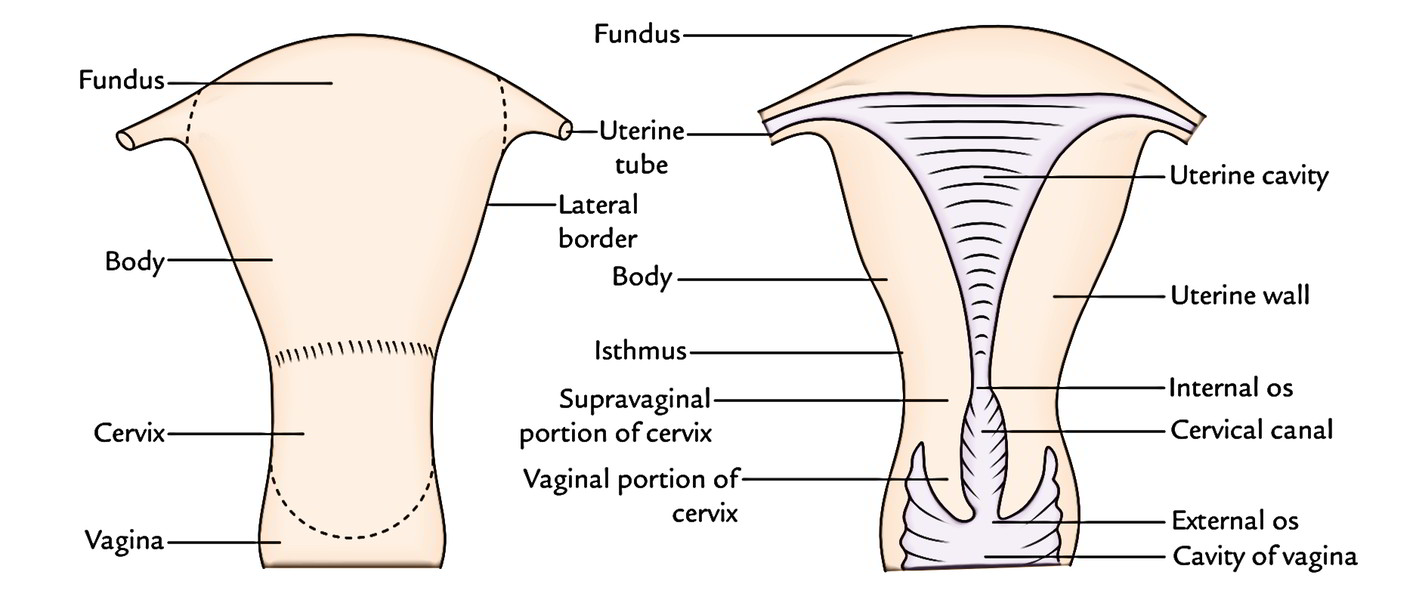
The uterus is comprised of two primary parts, which are as follows: (a) the large upper pearshaped part- the body and (b) a small lower cylindrical part- the cervix. The body creates upper 2/3rd of uterus and cervix creates the lower 1/3rd of the uterus. The part where the body and cervix meet, is marked by a circular constriction known as Isthmus. It’s well marked anteriorly. The uterine tubes are connected to the upper part of the body. The point of coalition between the uterine tube and body is named cornu of the uterus.
Body
The upper enlarged dome-like end of the body is termed fundus. It’s situated above the imaginary horizontal plane going through the openings of the uterine tubes. The fundus is convex on all sides and covered by the peritoneum.
The body stretches from the fundus to the isthmus and includes the uterine cavity. It’s flattened anteroposteriorly and presents anterior and posterior surfaces, and left and right lateral edges.
- Anterior surface: It’s flat and pointed downward and forward. It’s covered by the peritoneum up to the isthmus, where it’s reflected on to the upper surface of the urinary bladder creating the uterovesical pouch.
- Posterior surface: It’s convex and pointed upward and backwards. It’s covered by the peritoneum which stretches downward up to the posterior fornix of the vagina, where it’s reflected on the anterior aspect of rectum creating rectouterine pouch (or pouch of Douglas).
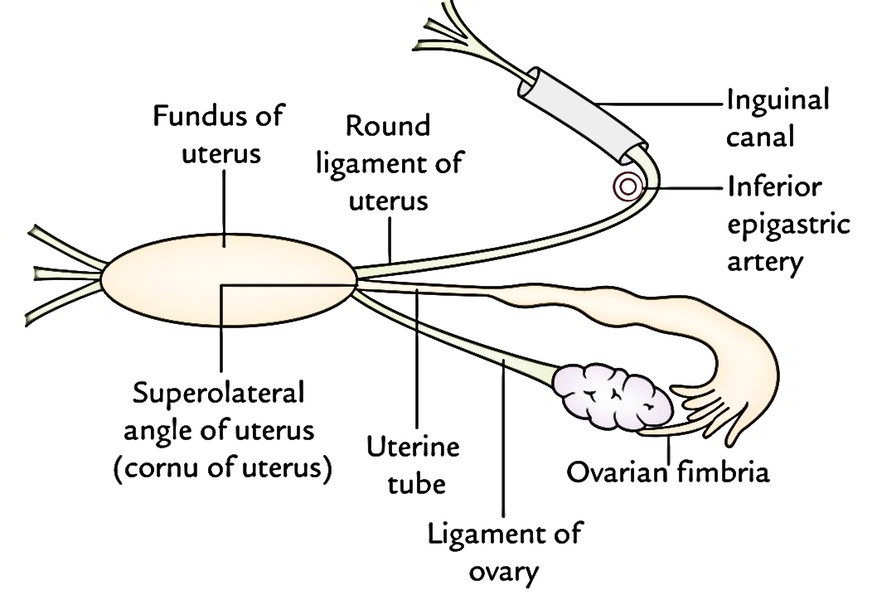
- Left and right lateral border: Every lateral border is rounded and related to the uterine artery. It’s nonperitoneal for it gives connection to the broad ligament of uterus. The uterine tube enters the uterus in the upper end of the border. Here the round ligament of the uterus is connected anteroinferior to the tube and the ligament of the ovary is connected posteroinferior to the tube.
Cervix
It’s the lower cylindrical part. Its lower part projects into the upper part of the vagina via its anterior wall. So, the cervix is split into 2 parts: (a) upper supravaginal part and (b) lower vaginal part.
Medically, the isthmus is composed by the upper 1-third (almost 0.8 millimeters) of the supravaginal cervix that is structurally quite similar to the uterus and creates what’s referred to as “lower uterine section” by the obstetricians.
Normal Position and Axes of The Uterus
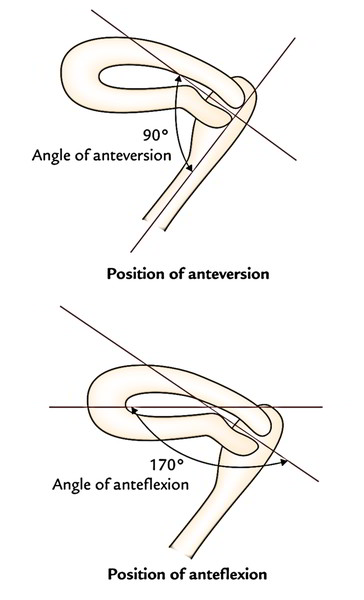
Normally the uterus is located in position of variation and anteflexion.
- Variation: The long axis of the cervix is normally bent forwards on the long axis of vagina creating an angle of about 90 °. This position is named the position of variation.
- Anteflexion: The long axis of the body of uterus is bent forward in the level of isthmus (internal os) on the long axis of cervix creating an angle of 170 °. This position of the uterus is referred to as anteflexion.
The angle of variation is a forward angle between the long axis of cervix and the long axis of vagina. It measures about 90 °
The angle of anteflexion is a forward angle between the long axis of the body of uterus and the long axis of the cervix in the isthmus. It measures about 170 °.
Relationships of The Uterus.
- Anteriorly:
- The body of uterus is associated with the uterovesical pouch and the superior surface of urinary bladder.
- The supravaginal portion of cervix is associated with the posterior surface of urinary bladder.
- The vaginal portion of cervix is associated with
- Posteriorly:
- The body of uterus is linked to the rectouterine pouch with coils of ileum and sigmoid colon in it.
- The supravaginal portion of cervix is associated with the rectouterine pouch with coils of ileum and sigmoid colon in it.
- Vaginal portion of cervix is related to posterior fornix
- Laterally:
- The body of uterus is related to the broad ligament and uterine artery and vein.
- The supravaginal portion of cervix is linked to the ureter and uterine artery.
- The vaginal portion of cervix is linked to the lateral fornices of the vagina
Cavity of The Uterus
The Cavity of Uterus Is Small In Comparison To Its Size Because of Its Thick Muscular Wall. It’s Split Into 2 Parts: Cavity of The Body And Cavity of The Cervix.
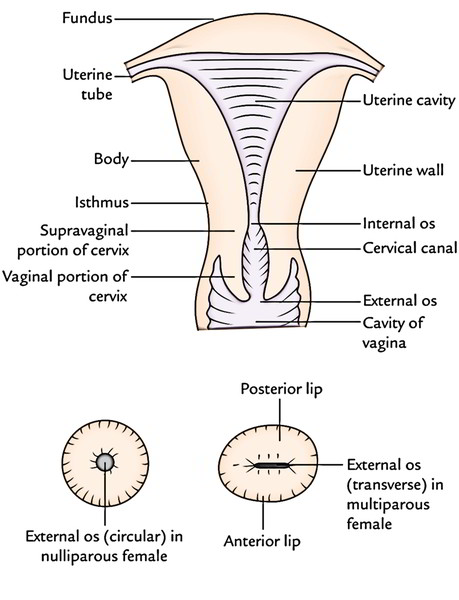
In the diagram below the upper part shows different parts of the uterus and lower part shows the shapes of external os in nulliparous and multiparous females.
Cavity of the Body (Uterine Cavity Suitable)
- It’s a triangular in coronal section (In the above figure upper part). The apex of the cavity is continuous below with the cervical canal via internal os. The implantation usually appears in the upper part of its posterior wall.
- it’s a simple slit in sagittal section, since the uterus is compressed anteroposteriorly and its anterior and posterior walls are just about in contact.
Cavity of The Cervix (Cervical Canal)
It’s A Spindle Shaped Canal, Being Wider In The Middle And Narrow At The Ends It Interacts Anterosuperiorly With The Cavity of Body of Uterus Via Internal Os And Inferiorly With The Cavity of Vagina Via External Os (Ostium Uteri)
In nulliparous women (women who’ve not given birth to a baby) the external os is small and circular, on the other hand in multiparous women (women who’ve given beginning to a couple of infants) the external os is large and transverse, and presents anterior and posterior lips (Lower Part in the above image).
Arbor Vitae Uteri
- Both anterior and posterior walls of the cervical canal present a longitudinal fold of mucous membrane. From every of these ridges a number of oblique folds such as the fronds of a palm leaf (plicae palmatae) ascend laterally, providing the look of branches from the stem of a tree, therefore the name arbor vitae uteri.
- The folds on the 2 walls aren’t opposed but match between 1 another (interlocking) so as to shut the cervical canal.
Ligaments
The ligaments of the uterus are classified into 2 types: false and true.
Ligaments of the uterus.
| False ligaments | True ligaments | ||
|---|---|---|---|
| Broad ligaments Rectouterine folds | Paired | Round ligaments Transverse cervical ligaments Uterosacral ligaments Pubocervical ligaments | Paired |
| Uterovesical fold (anterior ligament) Rectovaginal fold (posterior ligament) | Unpaired | ||
The fictitious ligaments are peritoneal folds while the true ligaments are fibromuscular groups. The bogus ligaments don’t supply support to the uterus while true ligaments supply support to the uterus.
Bogus Ligaments (Peritoneal Folds)
Broad Ligaments
All these really are the broad folds of peritoneum going from the side of the uterus to the lateral wall of the pelvis on every side.
Along with the uterus they create a septum across the pelvic cavity, splitting it into a small anterior part consisting of bladder and a large posterior part comprising rectum, coils of ileum, and sigmoid colon.
External Features
| Features | When the bladder is empty | When the bladder is distended |
|---|---|---|
| Two surfaces | Superior | Posterior surface |
| Inferior | Anterior surface | |
| Two borders | Anterior free border | Upper free border |
| Posterior attached border | Inferior attached border (base of broad ligament) |
Parts of The Broad Ligament
The broad ligament is subdivided into following 4 parts:
- Mesosalpinx: It’s the part of broad ligament between the fallopian tube and the ligament of the ovary.
- Mesometrium: It’s the part of broad ligament extending from the pelvic floor to the ovary, the ligament of ovary, and the body of uterus.
- Mesovarium: It’s the fold of posterior (or upper) layer of broad ligament extending to the ovary to be connected with that. It is located just below and behind the ampullary part of the uterine tube.
- Infundibulopelvic ligament (also termed suspensory ligament of ovary): It’s that part of the broad ligament which:
- Stretches from the infundibulum of the tube and the upper pole of the ovary to the lateral wall of the lesser pelvis.
- Includes the ovarian blood vessels, nerves, and lymph vessels.
- Is continued laterally over the external iliac vessels as a distinctive fold.
Contents of The Broad Ligament
The broad ligament includes these structures:
- 1 tube.
- Uterine tube.
- 2 ligaments.
- Round ligament of uterus.
- Ligament of ovary.
- 2 arteries.
- Uterine artery.
- Ovarian artery.
- 2 plexuses of nerves.
- Uterovaginal plexus.
- Ovarian plexus.
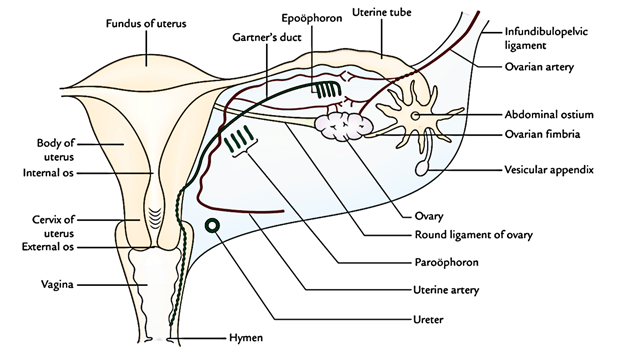
- 3 embryological remnants.
- Epoophoron and its duct (Gartner’s duct).
- Paroophoron.
- Vesicular appendices.
- Other structures.
- Lymph vessels and lymph nodes.
- Fibroareolar tissue.
- Uterovaginal and ovarian nerve plexuses.
Uterovesical Fold (Anterior Ligament)
It’s the fold of peritoneum, that is reflected from the very front of the uterus on to the upper surface of the bladder in the level of isthmus.
Rectovaginal Fold (Posterior Ligament)
It’s the fold of peritoneum that is reflected from the rear of the posterior fornix of vagina on to the front of rectum.
Rectouterine Fold
- On every side, it’s a semilunar fold of peritoneum stretching between the cervix and the rectum. It creates the lateral boundary of rectouterine pouch (of Douglas).
- Rectouterine pouch (of Douglas).
- It’s the most dependent part of the pelvic peritoneal cavity. It’s bounded in front by the supravaginal part of cervix and posterior fornix of vagina, behind by the middle third of the rectum, and on every side by the rectouterine fold. Its floor is located about 5.5 cm above the anal orifice and 7.5 cm above the vaginal orifice.
- The collection of pus or blood in this pouch can be taken out by providing an incision in the posterior fornix of vagina (posterior colpotomy).
True Ligaments (Fibromuscular Groups)
These ligaments provide support to the uterus, for this reason described under the heading, supports of the uterus.
Arterial Supply
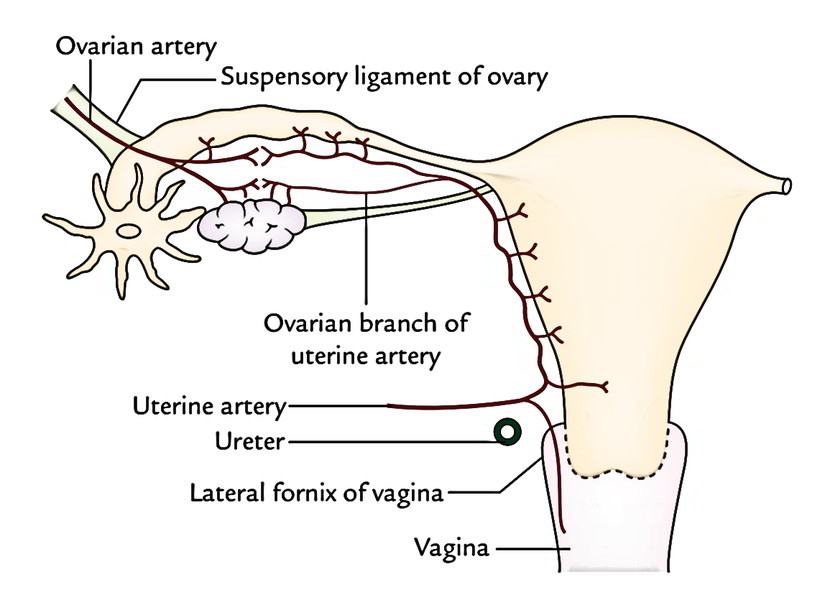
The uterus is provided primarily by 2 uterine arteries and partially by 2 ovarian arteries.
The uterine artery is a branch of anterior section of internal iliac artery. It runs medially across the pelvic floor in the base of the broad ligament, in the direction of the uterine cervix. It crosses the ureter from above lateral to the cervix above the lateral to the fornix of the vagina. Then it ascends along the side of the uterus. At the superolateral angle of uterus it turns laterally, runs along the uterine tube, and ends by anastomosing with the ovarian artery.
Branches and Distribution.
- Close to the cervix after crossing the ureter, it provides rise to ureteric, vaginal, and cervical branches. The cervical branches create circular anastomosis around the isthmus.
- Along the side of body of the uterus it produces arcuate (coronary) branches which run transversely on the anterior and posterior surfaces of the body of uterus and anastomoses with their counter parts along the midline.
- Along the fallopian tube it produces tubal branches and few ovarian twigs.
The uterine artery so provides uterus, vagina, medial 2-third of uterine tube, ovary, ureter, and structures inside the broad ligament.
Intrinsic uterine circulation
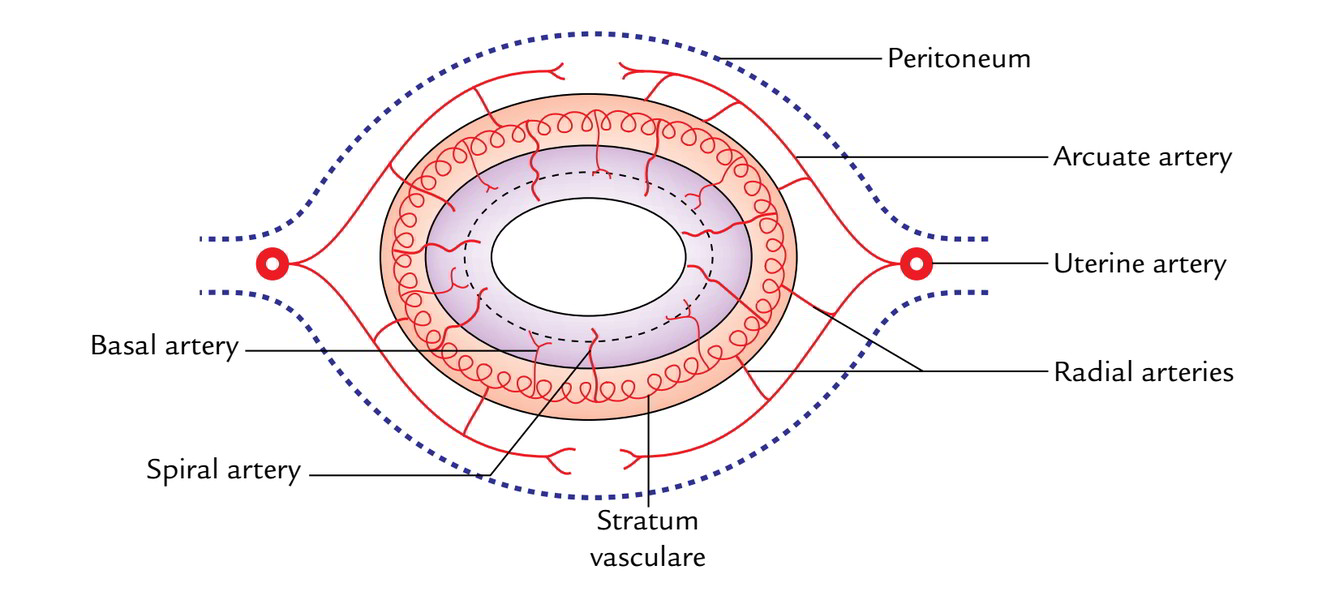
- The arcuate (coronary) arteries (branches of the uterine arteries) of 2 sides anastomose on the anterior and posterior surfaces of the body of the uterus in the midline.
- The radial arteries originate from the arcuate arteries and pierce the myometrium centripetally and anastomose with every other to create stratum vasculare in the middle layer of muscular coating.
- From stratum vasculare, 2 sets of branches, basal and spiral, originate to provide the endometrium. The functional zone of the endometrium that is cast off during menstruation is provided by the spiral arteries, on the other hand the basal zone of the endometrium which helps in the regeneration of the denuded endometrium is provided by the basal arteries.
Venous Drainage
The veins of the uterus correspond to arteries. They create venous plexus along the lateral edges of the uterus, which empties into internal iliac veins via uterine and vaginal veins.
Lymphatic Drainage
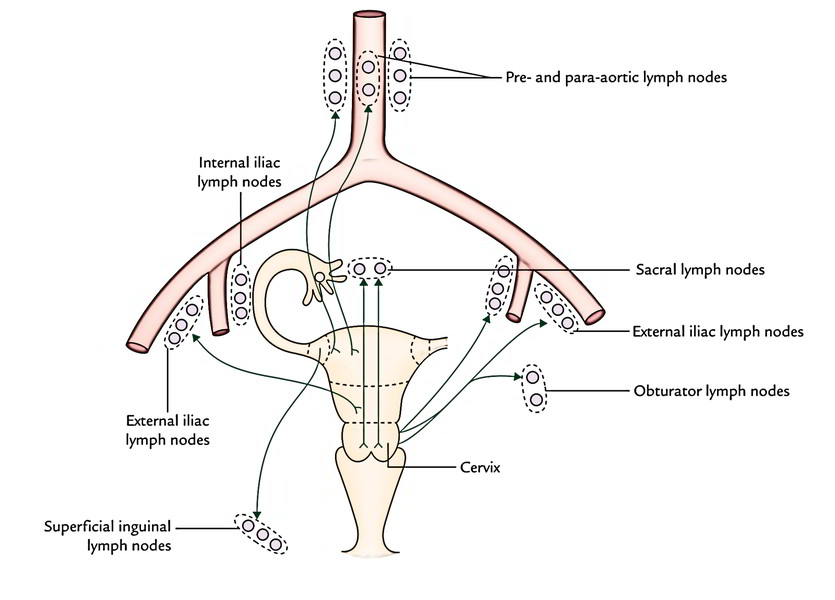
The lymphatic drainage of the uterus is medically essential because uterine cancer spreads via lymphatics. The lymphatic drainage takes place as follows:
- From fundus and upper part of the body, the majority of the lymphatics drain into pre and para-aortic lymph nodes along the ovarian vessels. Nevertheless, a few lymphatic vessels from the lateral angles of the uterus drain into superficial inguinal lymph nodes along the round ligaments of the uterus.
- From the lower part of the body, the lymph vessels drain into external iliac nodes via broad ligament.
- From cervix, on every side the lymph vessels drain in 3 ways:
1. Laterally, the lymph vessels drain into external iliac and obturator nodes by passing parametric tissue, few of these vessels are intercepted by paracervical nodes.
2. Posterolaterally, the lymph vessels drain into internal iliac nodes by passing along the uterine vessels.
3. Posteriorly, the lymph vessels drain into sacral nodes by passing along the uterosacral ligaments.
Nerve Supply
The uterus is richly innervated by both sympathetic andparasympathetic fibres.
- The sympathetic fibres are originated from T12 L2 spinal sections. The sympathetic fibres cause uterine contraction and vasoconstriction.
- The parasympathetic fibres are originated from S2 S4 spinal sections. The parasympathetic fibres inhibit the uterine muscles and cause vasodilatation.
Strictly speaking, the autonomic management of uterine tasks is meager. Actually the uterine tasks are mainly under hormonal control.
- Visceral afferents taking pain from the uterus take 2 pathways:
- From the body of uterus, they follow sympathetic nerve pathways. Consequently, pain connected with uterine spasm is referred to the T12 L2 dermatomes (example, midback, pubic and inguinal regions, and anteromedial aspect of the thigh).
- From the cervix, they cause along the pelvic splanchnic nerves, thus pain related to cervical dilatation is referred to the sacral dermatomes (example, perineum, gluteal region, and posterior aspect of the thigh).
Structure
The wall of the body of uterus is composed of 3 layers. From superficial to deep these are:
- Perimetrium: It’s peritoneal covering of the uterus originated from broad ligament.
- Myometrium: It’s the thickest layer and is composed of compactly arranged smooth muscle bundles.
- Endometrium: It’s the mucosal lining of the body of the uterus. It demonstrates cyclic changes.
The structure of cervix differs from body for it’s not lined by the endometrium and it doesn’t reveal cyclic changes.
Supports of The Uterus
The uterus is kept in position and prevented from sagging down by a number of structures supplying support to it. The supports of the uterus are subdivided into 2 types: main or primary supports and accessory or secondary supports.
Primary Supports
- Muscular.
- Pelvic diaphragm.
- Perineal body.
- Urogenital diaphragm.
- Visceral.
- Urinary bladder.
- Vagina.
- Uterine axis.
- Fibromuscular.
- Transverse cervical ligaments (of Mackenrodt).
- Pubocervical ligaments.
- Uterosacral ligaments.
- Round ligaments of the uterus.
Secondary Supports
- Broad ligaments.
- Uterovesical fold of peritoneum.
- Rectovaginal fold of peritoneum.
Transverse Cervical Ligaments (Mackenrodt’s Ligaments)
- They may be the most significant ligaments of the uterus, for this reason frequently termed cardinal ligaments. They’re created by the condensation of pelvic fascia around the uterine vessels.
- Every ligament creates a fan-shaped fibromuscular group which stretches from the lateral aspect of cervix and upper vaginal wall to the lateral pelvic wall. They create a hammock which supports the uterus and prevent its downward displacement.
- The tightening of Mackenrodt’s ligament is often done in surgical repair of the prolapsed uterus.
Pubocervical Ligaments
All these are a pair of fibrous bands which go from the cervix to the posterior aspects of the pubic bones, along the inferolateral surfaces of the urinary bladder. They correspond to puboprostatic ligaments in male.
Uterosacral Ligaments
- All these are a pair of fibrous bands which go from the cervix to the 2nd and third sacral vertebrae, and pass on every side of the rectum.
- They are located underneath the rectouterine folds of peritoneum which create the lateral borders of the rectouterine pouch.
- These ligaments pull the cervix backwards against the forward pull of the round ligaments and help in the maintenance of bend and anteverted Positions of the uterus.
Round Ligaments of The Uterus (Ligament Teres Uteri)
All these are a pair of long (10-12 cm) fibromuscular bands which be located between the 2 layers of broad ligament.
Every ligament starts at the lateral angle of the uterus, enters forward and laterally between both layers of broad ligament, enters the deep inguinal ring after winding around the lateral side of the inferior epigastric artery. It traverses the inguinal canal, appears via the superficial inguinal ring, and rips into numerous threadlike fibrous groups which unite with the fibroareolar tissue of the labium majus.
These ligaments pull the fundus forwards and help keep the variant and anteflexion of the uterus.
Clinical Significance
Cervical Carcinoma
It’s the most frequently encountered cancer in females (11%). The second commonest cancer in females is breast cancer (about 8%). It’s uncommon before 20 years old and reaches its peak between the ages 45 and 55 years. 80% cervical cancers are squamous cell carcinoma and are related to sex. Early sexual exposure and promiscuity are notable variables.
It distributes directly to adjacent structures and metastasizes via lymphatics to pelvic lymph nodes and after that to the preaortic and para-aortic lymph nodes.
Clinical Features
- Abnormal vaginal bleeding especially intermenstrual.
- Postcoital bleeding.
- Pain, anorexia, and weight reduction.
- Fibroids/fibromyomas of uterus: These are benign tumors originating from myometrial cells. They can be seen in about 1 fifth of women above 35 years old. They’re often multiple and could go through degenerative charges. They go through atrophy after menopause. Medically they present as abnormal bleeding (hypermenorrhea) and unusual contour of the uterus on bimanual palpation. They’re frequently asymptomatic. Small asymptomatic fibroids require no treatment. If large, hysterectomy (removal of uterus) is the treatment of choice.
- Caesarean section: It’s the surgical procedure for delivering the baby by cutting open the abdomen and uterus in cases where vaginal delivery isn’t possible. The term caesarean section is thus termed since the Roman Emperor Julius Caesar was allegedly born by this surgical procedure.

 (54 votes, average: 4.61 out of 5)
(54 votes, average: 4.61 out of 5)