Among the 3 pairs of salivary glands, viz. parotid, submandibular and sublingual, the parotid (para = around, otic = ear) gland is the largest. It’s composed just about wholly of serous alveoli. It weighs about 25 grams. It’s lobulated and yellowish brown.
Location
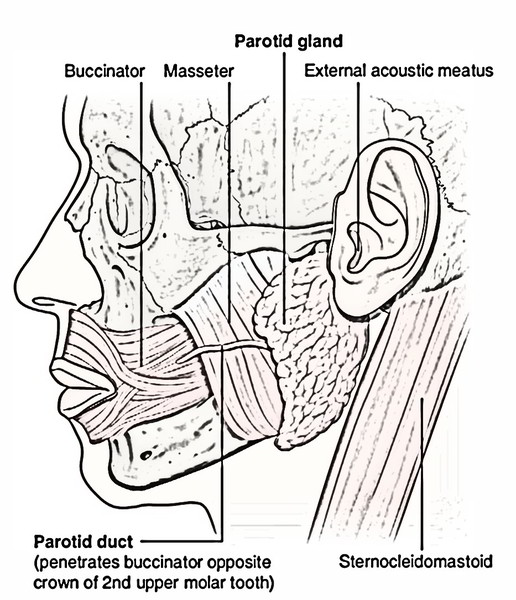
It is location is in the pyramidal fossa, posterior to the ramus of the mandible named retromandibular fossa (parotid bed).
Bounds of the Parotid Bed
It’s bounded:
- Anteriorly: by the posterior border of the ramus of mandible.
- Posteriorly: by the mastoid process.
- Superiorly: by the external acoustic meatus and posterior part of temporomandibular joint.
- Medially: by styloid process.
The parotid bed is lined by muscles, likely to allow it to be soft as under:
- Ramus of the mandible is covered by 2 muscles: masseter laterally and the medial pterygoid medially.
- Mastoid process is covered by 2 muscles: sternocleidomastoid laterally and posterior belly of digastric muscle medially.
- Styloid process is enveloped by 3 slight muscles: styloglossus, stylopharyngeus and stylohyoid.
- The parotid gland is too soft to be felt in healthy individual but 1 can identify the bony borders of the parotid bed.
Extent
The parotid gland being soft isn’t confined only to the parotid bed but goes beyond it. The extent of parotid gland is as follows: it goes from external auditory meatus above, to the upper part of the carotid triangle below; medially it goes to the styloid process (close to the side wall of pharynx) and wraps around the neck of the mandible. Posteriorly it overlaps the sternocleidomastoid muscle and anteriorly it goes over the masseter for a varying space. A part of the forward extension is frequently detached from the remaining part of the gland and is referred to as accessory parotid gland The accessory parotid gland is located between the zygomatic arch above and the parotid duct below. Several ducts from accessory gland open into the parotid duct.
Parotid Capsule (Or Parotid Sheath)
The parotid gland is enclosed in a fibrous capsule named parotid capsule.
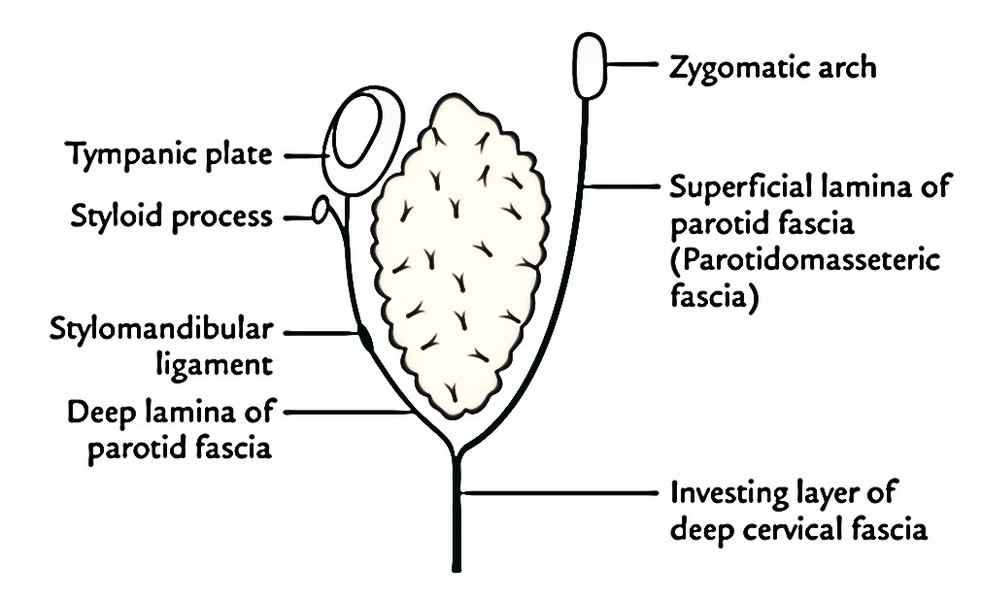
It’s created by the tough investing layer of deep cervical fascia. This fascia divides in the region between the angle of the mandible and mastoid process to enclose the gland. The superficial lamina is thick, powerful, unyielding and adherent to the gland while deep lamina is thin. The superficial lamina combines with the epimysium of masseter to create a thick parotidomasseteric fascia that is connected above to the zygomatic arch. The thin deep lamina is connected to the tympanic plate and styloid process of the temporal bone; it thickens to create stylomandibular ligament, which divides the parotid gland from the submandibular gland.
Clinical Significance
Infection of the parotid gland: The parotid gland is usually infected by the mumps virus causing inflammation and swelling of the gland (mumps).
The parotid swellings are extremely painful because of unyielding temperament of the parotid capsule, any inflammation or pressure inside the parotid gland will cause acute pain. This is caused by the stretching of the capsule and stimulus of branches of great auricular nerve. The pain is normally exacerbated at meal time when gustatory stimulation to gland results in increased parotid secretion enriching additional turgor inside the capsule. Nevertheless, patient is relieved of pain to some degree after taking meals because of release of secretions. This is viewed regularly in patients suffering from mumps.
External Features
The gland resembles a 3-sided pyramid with apex pointed downwards. It presents these features:
- An apex
- 4 surfaces
- Superior surface or base
- Superficial surface
- Anteromedial surface
- Posteromedial surface
3 edges
- Anterior.
- Posterior.
- Medial.
Connections
Apex
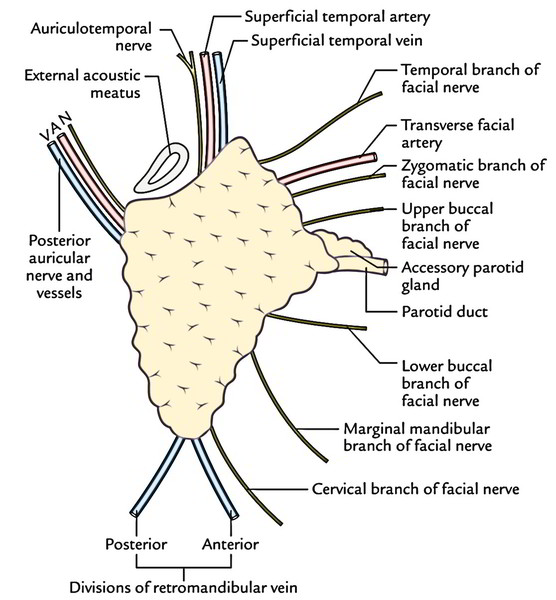
It projects downwards overlapping the posterior belly of digastric muscle and adjoining part of the carotid triangle. The structures appearing via the apex contain:
- Cervical branch of the facial nerve.
- Anterior and posterior sections of retromandibular vein.
Superior Surface or Base
It’s concave and related to the external acoustic meatus and posterior aspect of temporomandibular joint.
These structures appear via it:
- Superficial temporal vessels
- Auriculotemporal nerve
Superficial Surface
It’s the largest of the 4 surfaces. It’s covered from superficial to deep by:
- Skin
- Superficial fascia featuring anterior branches of greater auricular nerve, superficial parotid (preauricular) lymph nodes and platysma
- Parotid fascia
- Deep parotid lymph nodes embedded in the gland
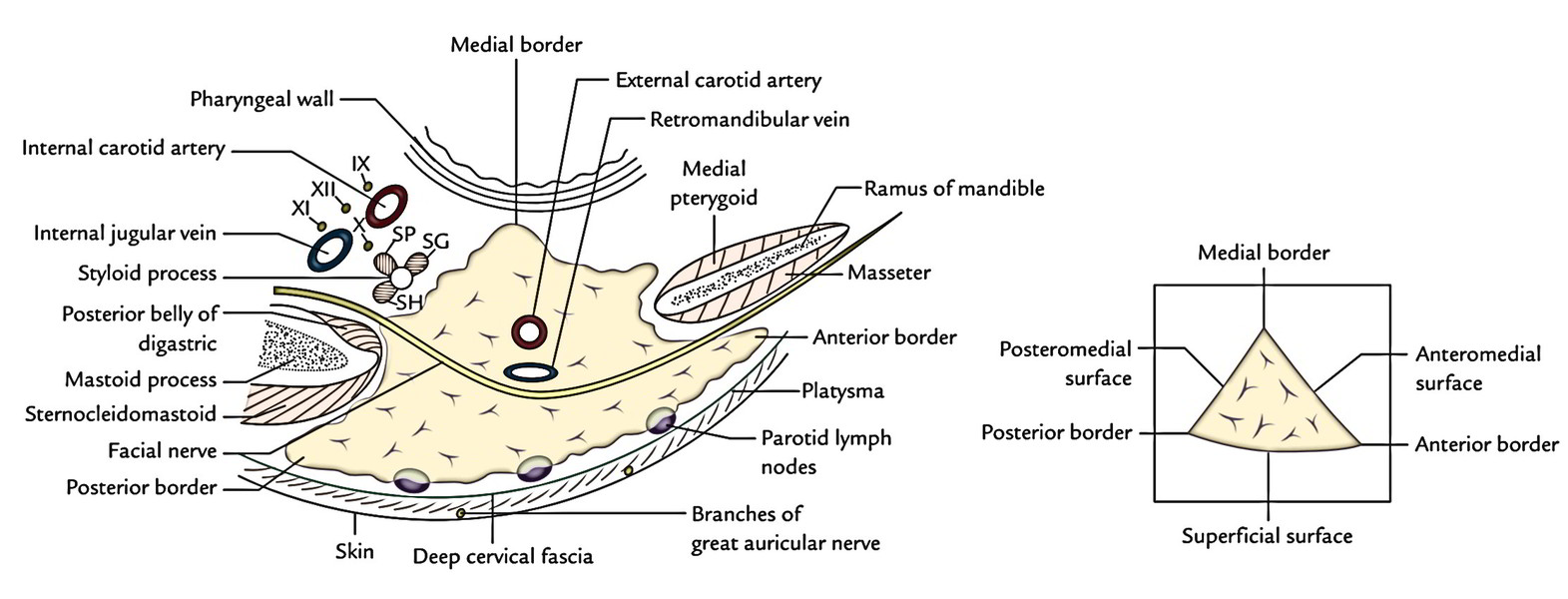
Anteromedial Surface
It’s deeply grooved by the posterior border of the ramus of the mandible. It’s related to:
- Masseter
- Medial pterygoid
- Posterior border of the ramus of the mandible
- Lateral aspect of the temporomandibular joint
- The branches of facial nerve issue on face from underneath the anterior margin of the surface
Posteromedial Surface
- It’s moulded onto the mastoid and styloid processes and their covering muscles. Hence it’s related to:
- Mastoid process, sternocleidomastoid and posterior belly of digastric.
- Styloid process and styloid group of muscles.
The styloid process and its muscles divide the gland from internal carotid artery, internal jugular vein and last 4 cranial nerves.
These structures goes into the gland via this surface:
- Facial nerve trunk in its upper part
- External carotid artery in its lower part
Anterior Border
It divides the superficial surface from the anteromedial surface. These structures (from above downwards) come in a radiating manner underneath this border:
- Temporal branch of the facial nerve
- Zygomatic branch of the facial nerve
- Transverse facial vessels
- Upper buccal branch of the facial nerve
- Parotid duct
- Lower buccal branch of the facial nerve
- Fringy mandibular branch of the facial nerve
Posterior Border
It divides the superficial surface from the posteromedial surface.
These structures appear underneath this border:
- Posterior auricular vessels
- Posterior auricular branch of the facial nerve
Medial Border
It splits the anteromedial surface from the posteromedial surface. It’s related to the lateral wall of the pharynx.
Structures Present Inside the Parotid Gland
3 chief structures either in part or in whole traverse the gland and branch inside it. From superficial to deep these are:
- Facial nerve.
- Retromandibular vein.
- External carotid artery.
Some members of the deep parotid lymph nodes and filaments of auriculotemporal nerve are also found inside the gland
The Facial Nerve
The facial nerve is most superficial. It enters the gland via the upper part of the posteromedial surface and breaks up into its terminal branches inside the gland. The branches run horizontally and leave the gland via its anteromedial surface and appear on the face by passing underneath its anterior border.
The 5 terminal branches of the facial nerve radiate like a goose foot via the anterior border of the gland and supply the muscles of facial expression. Such branching pattern of the facial nerve is referred to as pes anserinus.
The Retromandibular Vein
The retromandibular vein takes up the intermediate zone of the gland and is composed by the unification of the superficial temporal and maxillary veins. It finishes below by splitting into anterior and posterior sections. The anterior section joins the facial vein to create the common facial vein while posterior section joins the posterior auricular vein to create the external jugular vein.
The External Carotid Artery
The external carotid artery pierces the lower part of the posteromedial surface to goes into the gland where it inhabits the deep zone of the gland. Inside the gland it breaks up into superficial temporal and maxillary arteries. The transverse facial artery, branch of superficial temporal artery issues via the anterior border of the gland
Patey’s Faciovenous Plane
The parotid gland is split into large superficial and small deep parts or lobes. These lobes are joined by the isthmus of the glandular tissue, so the gland appears H shaped (shaped like a collar stud) in coronal segment. The branches of facial nerve enter forwards via the isthmus. The plane between the superficial and deep lobes where nerves and veins are located has been designated by Patey as faciovenous plane. This plane helps the surgeons to eliminate the parotid tumor without damaging the nerve.
Clinical Significance
Amalgamated parotid tumor: It’s slow-growing lobulated painless tumor of large superficial part of the parotid gland It’s so called due to its combined histological look. Now it’s called pleomorphic adenoma. After several years of slow benign increase, it might go through a malignant change.
Parotid Duct (Stenson’s Duct)
Parotid duct, about 5 cm long, appears from the middle of the anterior border of the gland and opens into the vestibule of the mouth opposite the crown of upper second molar tooth.
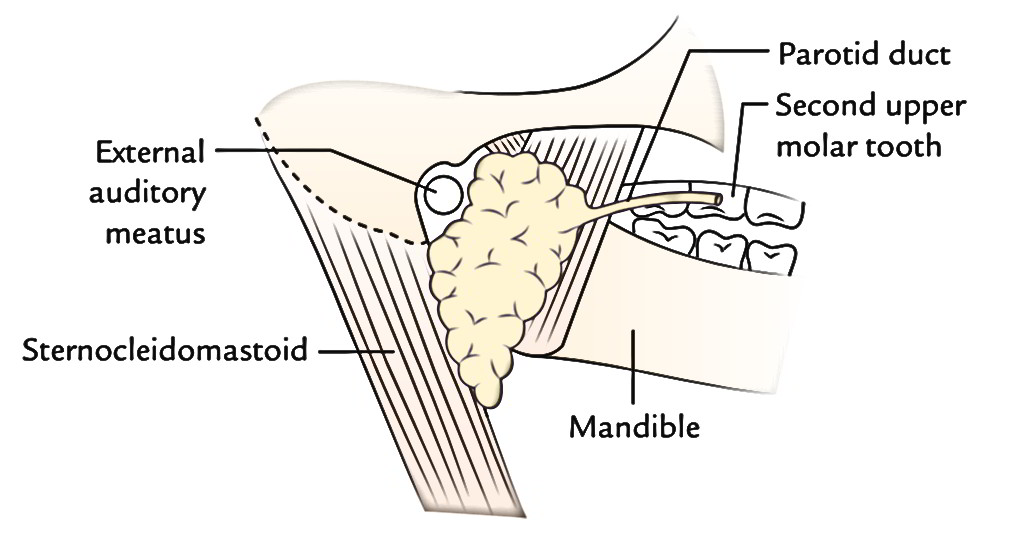
Course
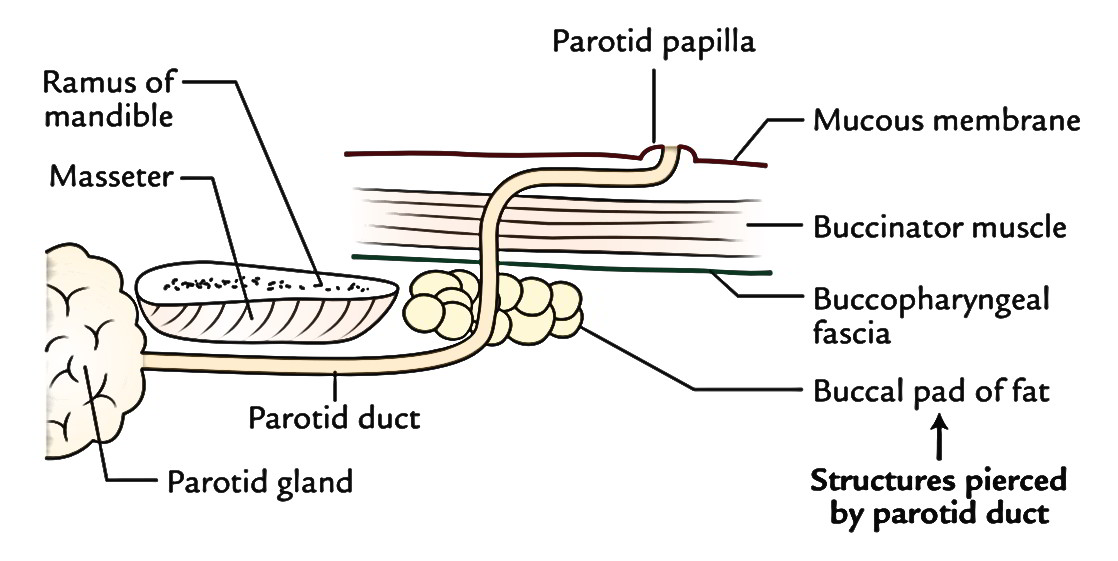
The course taken by the duct is as follows: After appearing from the gland, it runs forwards over the masseter between the upper and lower buccal branches of the facial nerve; at the anterior border of masseter, it suddenly turns inwards, practically at 90 ° (first bending) and pierces buccal pad of fat, buccopharyngeal fascia and buccinator muscle.
After piercing the buccinator muscle, the parotid duct runs forwards (second curve) for about 1 cm between it and the buccal mucosa. Eventually, the duct turns medially (third bending) and opens into the vestibule of mouth opposite the crown of upper second molar teeth. This tortuous course of the duct gives a valve-like mechanism to stop the inflation of the duct system of parotid gland during excessive blowing of the mouth as in trumpet blowing.
Surface Anatomy of the Parotid Duct
On the face the parotid duct is represented by the middle third of the line going from lower border of tragus to the midpoint between the ala of the nose and the red margin of the upper lip.
The accessory gland is emptied by a small duct that opens into the upper aspect of the parotid duct.
Clinical Significance
The probing of the parotid duct is hard due to its tortuous course. The probe is held in the sharp curves of the duct.
The parotid duct is located 1 finger’s breadth below the zygomatic arch and when the teeth are clenched, it might be rolled up and down against the stressed masseter.
The parotid duct being a superficial structure on the face, might be damaged in injuries to the face or might be cut accidentally during surgical procedures on the face.
The parotid duct and its ramifications can be demonstrated radiologically by injecting radio-opaque dye via a fine needle or canula inserted into the mouth of the duct in the vestibule of the oral cavity (parotid sialogram).
Sometimes, calculi (stones) may create in the parotid gland and parotid duct. The calculi lodged in the distal portion of the gland could be taken out by splitting up the duct from its opening in the mouth.
Nerve Supply
The parotid gland is supplied by the parasympathetic, sympathetic and sensory fibres:
Parasympathetic (secretomotor) supply: It is supplied via auriculotemporal nerve. The preganglionic fibres originate from the inferior salivatory nucleus in the medulla and pass successively via glossopharyngeal nerve, tympanic branch of glossopharyngeal (Jacobson’s nerve), tympanic plexus and lesser petrosal nerve to relay into otic ganglion. Postganglionic fibres originate from the cells of the ganglion and go through the auriculotemporal nerve to furnish the parotid gland. The stimulation of parasympathetic supply creates watery secretion.
Sympathetic supply: It’s originated from sympathetic plexus around external carotid artery created by postganglionic fibres originated from superior cervical sympathetic ganglion. The preganglionic sympathetic fibres originate from the lateral horn of T1 spinal section. The sympathetic fibres are vasomotor and their stimulus creates thick sticky secretion.
Sensory Supply: It’s originated from:
- Auriculotemporal nerve.
- Great auricular nerve (C2 and C3).
- The C2 fibres are sensory to the parotid fascia.
Clinical Significance
Frey’s syndrome (auriculotemporal nerve syndrome):
Occasionally penetrating wounds of the parotid gland may damage auriculotemporal and great auricular nerves. The auriculotemporal nerve includes parasympathetic (secretomotor), sensory and sympathetic fibres. The great auricular nerve includes sensory and sudomotor fibres. When these nerves are cut, during regeneration the secretomotor fibres grow into endoneurial sheaths of fibres supplying cutaneous receptors for pain, touch and temperature and sympathetic fibres supplying sweat glands and blood vessels. Hence a stimulation meant for salivation evokes cutaneous hyperesthesia, perspiration and flushing. The presenting features of Frey’s syndrome are:
When an individual eats, the ipsilateral cheek (parotid region) becomes red, hot and debilitating. It’s related to beads of perspiration (gustatory sweating).
When someone shaves, there’s cutaneous hyperesthesia in front of the ear.
Vascular Supply
The arterial supply of parotid gland is originated from the external carotid and superficial temporal arteries.
The venous drainage of parotid gland happens into retromandibular and external jugular veins.
Lymphatic Drainage
The lymphatics from the parotid gland drain into the superficial and deep parotid lymph nodes, which in turn drain into deep cervical lymph nodes. The superficial parotid nodes are located in the superficial fascia over the gland and deep nodes, deep to parotid capsule. Few members of the group are located in the superficial zone of the parotid gland
Development
The parotid gland is ectodermal in origin. The parotid primordium grows during the 6th week of intrauterine life as a cord of cells by proliferation of ectodermal lining of the vestibule of the mouth near the angle of archaic oral fissure. It grows backwards in the direction of the ear and branches repeatedly. The parotid bud and its branches canalize to create the duct system and acini.
All the salivary glands originate from proliferation of the oral epithelium. Out of the 3 pairs of large salivary glands only parotid glands grow from ectoderm, others (submandibular and sublingual) grow from endoderm.

 (71 votes, average: 4.30 out of 5)
(71 votes, average: 4.30 out of 5)