As it creates different fascial spaces in the neck, the deep cervical fascia of the neck is medically very significant. Capsules to the glands and invests the muscles in the region are also given by it. Moreover, around neurovascular structures, it forms protective sheath. To steer the spread of infection or pus in the neck, the layers of deep cervical fascia create fascial planes. 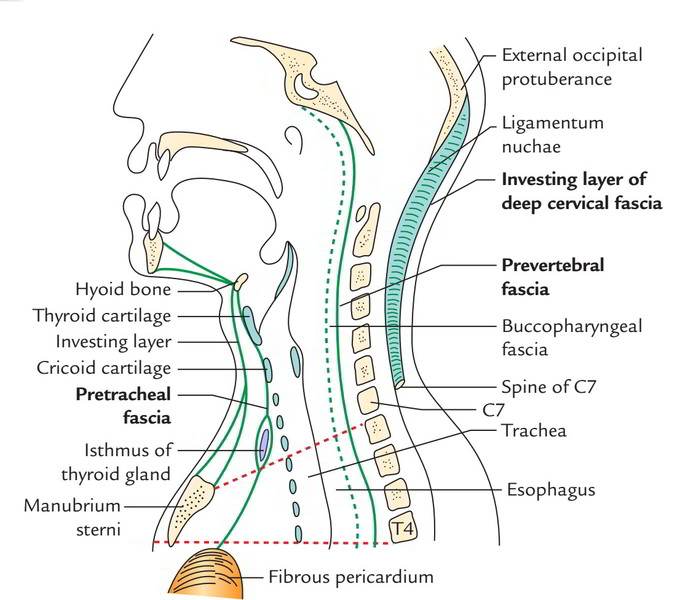
 The deep cervical fascia of the neck is composed of 3 layers. From outside inwards these are as follows:
The deep cervical fascia of the neck is composed of 3 layers. From outside inwards these are as follows:
- Investing layer of deep cervical fascia.
- Pretracheal fascia.
- Prevertebral fascia.
The spaces among the structures of the neck are filled up with loose areolar tissue. The structures of the neck are largely destined to move up and down. The layers of deep cervical fascia are no more in relation to the laminar conholesation of loose areolar tissue generated by the movements of these structures. These laminar conholesations take different names in different regions and are constant with every other either directly or indirectly via loose areolar tissue. The free areolar tissue creates fascial sheets or laminae in exactly the same way as unwoven cotton creates sheets of material after spinning. These laminae ensheath muscles and other moving structures. This allows movement between the sheaths and movements of structures inside them. 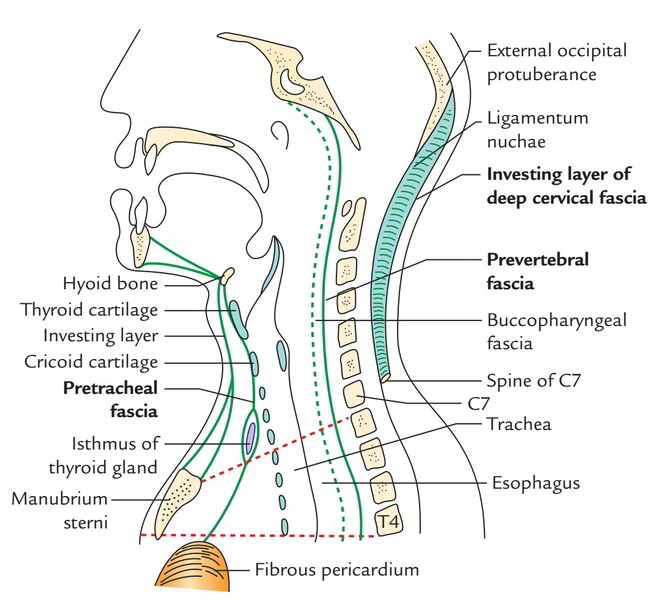
Investing Fascia
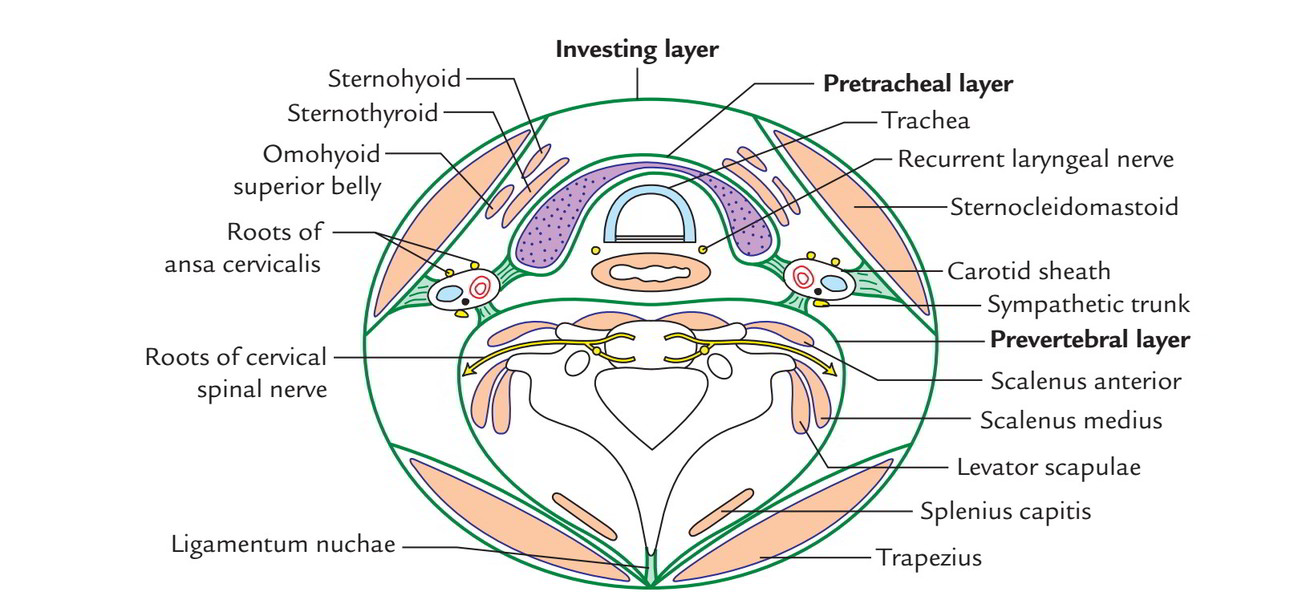
This layer encircles the neck like a collar, deep to platysma and superficial fascia. In doing so it encloses the sternocleidomastoid and trapezius– the 2 large superficial muscles on each side of the neck.
Attachments
Superiorly it’s connected to external occipital protuberance, superior nuchal line, mastoid process and lower border of mandible from behind forwards. Inferiorly it’s connected to the spine of scapula, acromion process, upper aspect of clavicle and jugular notch of manubrium sterni from behind forwards. Anteriorly through the midline, it becomes constant with its counter part of the other side. In the anterior midline it’s connected to symphysis menti, hyoid bone jugular notch from above downwards. Posteriorly it’s connected to ligamentum nuchae and spine of 7th cervical vertebra.
Outlining of the Investing Layer
Vertical tracing: When delineated upwards above the hyoid bone, it splits to enclose the submandibular salivary gland The superficial layer covers the superficial outermost layer of the gland and it’s connected to the lower border of the body of the mandible. The deep layer covers the medial outermost layer of the gland and is connected to the mylohyoid line of the mandi-ble. Posterior to the submandibular gland, at the lower pole of the parotid gland, it divides to enclose this gland as well. 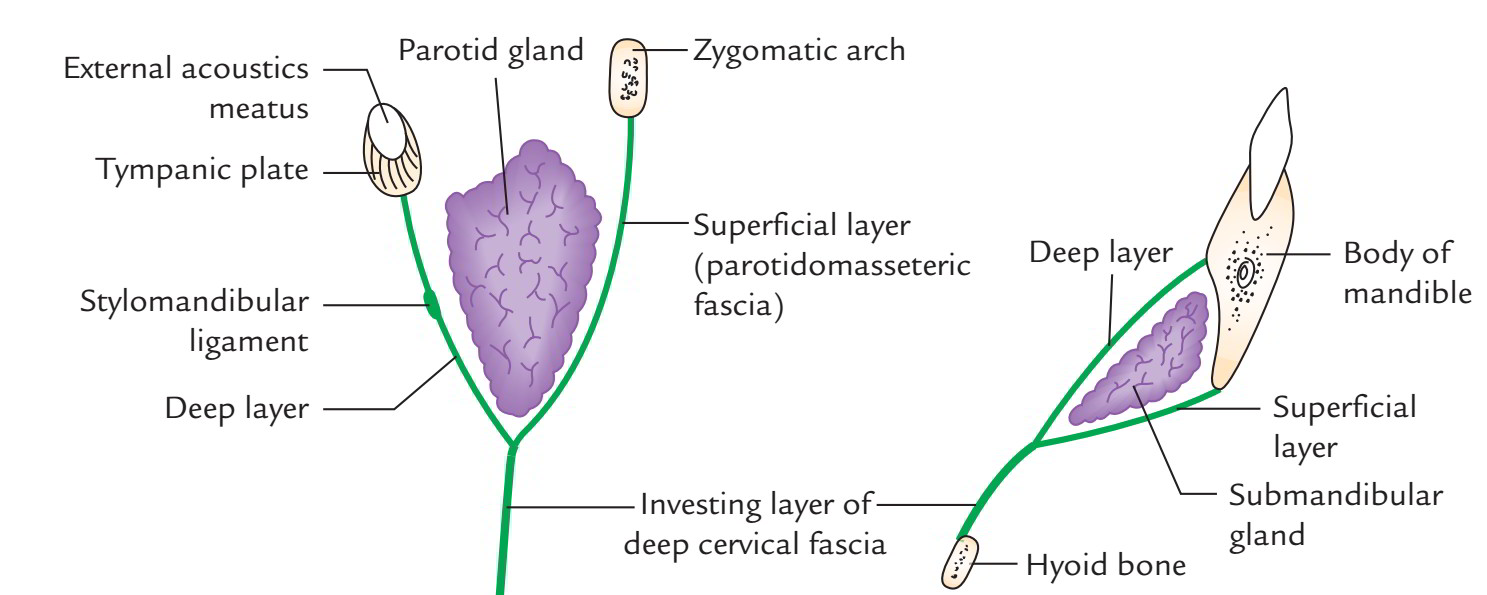 The superficial layer is powerful and covers the superficial surface of the parotid gland as parotidomasseteric fascia to get connected to the lower border of the zygomatic arch. The deeper layer enters deep to the parotid gland to get connected to the lower border of the tympanic plate and styloid process of the temporal bone. The part of the layer extending between the styloid process and the angle of mandible conholeses to create the stylomandibular ligament which divides the parotid gland from submandibular gland When followed downwards, the fascia divides twice to enclose 2 spaces: Above the suprasternal notch, it divides into 2 layers to enclose suprasternal space (of Burns) before being connected to the anterior and posterior edges of the suprasternal notch. The suprasternal space includes:
The superficial layer is powerful and covers the superficial surface of the parotid gland as parotidomasseteric fascia to get connected to the lower border of the zygomatic arch. The deeper layer enters deep to the parotid gland to get connected to the lower border of the tympanic plate and styloid process of the temporal bone. The part of the layer extending between the styloid process and the angle of mandible conholeses to create the stylomandibular ligament which divides the parotid gland from submandibular gland When followed downwards, the fascia divides twice to enclose 2 spaces: Above the suprasternal notch, it divides into 2 layers to enclose suprasternal space (of Burns) before being connected to the anterior and posterior edges of the suprasternal notch. The suprasternal space includes:
- Sternal heads of sternocleidomastoid muscles,
- Jugular venous arch,
- Interclavicular ligament and
- Lymph node (occasionally).
Above the middle third of clavicle, it divides into 2 layers to enclose the supraclavicular space. The anterior and posterior layers get connected to the anterior and posterior edges of the upper surface of the clavicle. The posterior layer encloses the inferior belly of omohyoid and after being connected to clavicle it becomes continuous with the posterior layer of clavipectoral fascia. 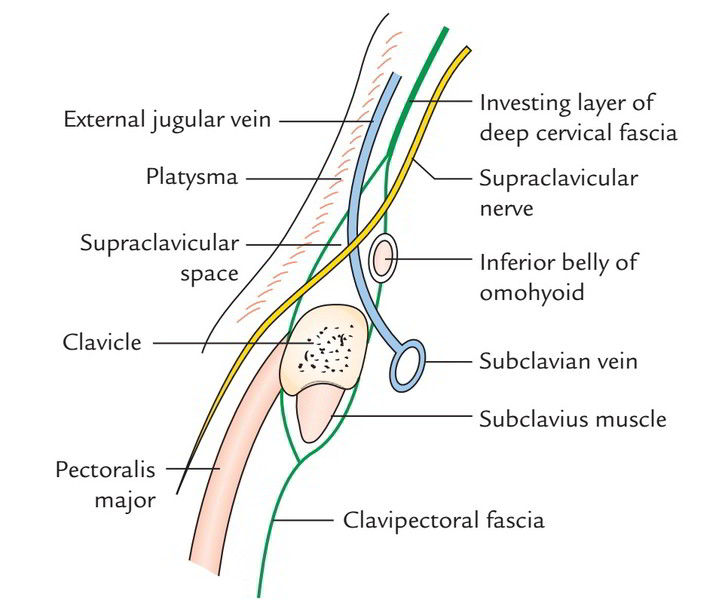 The supraclavicular space includes:
The supraclavicular space includes:
- Terminal part of the external jugular vein and
- Supraclavicular nerves until they get cutaneous.
The investing layer also creates fascial pulleys to anchor the tendons of the digastric and omohyoid muscles. Horizontal tracing: When delineated forwards from its connection to ligament nuchae, it first splits to enclose the trapezius, subsequently creates the roof of the posterior triangle, then again splits to enclose the sternocleidomastoid and ultimately creates the roof of the anterior triangle. ‘Rule of 2’: When summed up, it’s noted that investing layer of deep cervical fascia presents everything in ‘2’, for example it encloses 2 muscles, trapezius and sternocleidomastoid creates roofs of 2 triangles, anterior and posterior triangles divides to enclose 2 glands, submandibular and parotid divides to enclose 2spaces, suprasternal and supraclavicular creates 2 fascial slings (pulleys) for inferior belly of omohyoid and intermediate tendon of digastric muscle.
Pretracheal Fascia
This layer of deep cervical fascia covers the front and sides of trachea, thus its name- pretracheal fascia. It splits to enclose the thyroid gland creating its capsule and is connected to the oblique line of thyroid cartilagevand to the arch of cricoid cartilage anteriorly. A fibrous group termed ligament of Berry is originated from this fascia and attaches the capsule of the lateral lobe of the thyroid gland to the cricoid cartilage. 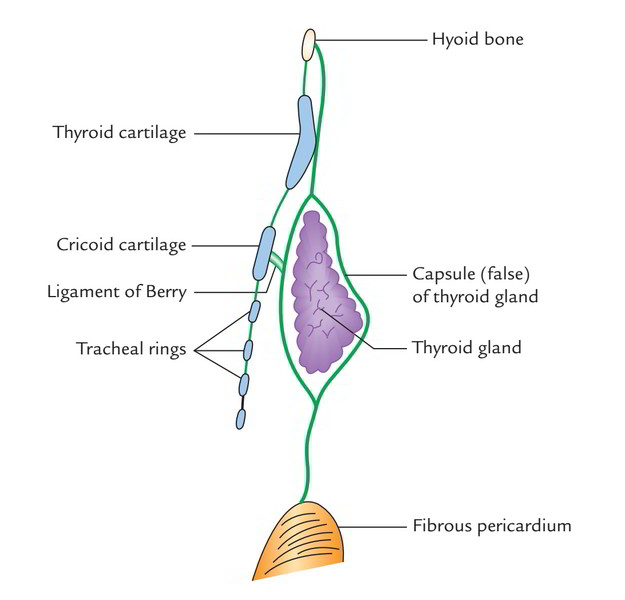
Delineating of the Pretracheal Fascia
Horizontal tracing: When followed horizontally, it unites with all the investing layer of deep cervical fascia enclosing the sternocleidomastoid and the anterior wall of the carotid sheath. Vertical tracing: When outlined above, it’s connected to the hyoid bone and when outlined below, it enters the thorax in front of the trachea and fusion with the apex of the fibrous pericardium. Clinical significance The connection of pretracheal fascia to hyoid bone and thyroid and cricoid cartilages enables the thyroid gland to move up and down with the larynx during swallowing. The layers of pretracheal fascia which cover the posterior surface of the thyroid lobe is ill defined. Because of this, enlarged thyroid (goitre) easily bulges posteriorly to compress the esophagus causing dysphagia. The pretracheal fascia gives a slick surface to enable free movements of trachea during swallowing.
Prevertebral Fascia
It’s incredibly powerful and is located in front of the prevertebral muscles.
Delineating of the Prevertebral Fascia
Horizontal tracing: When followed laterally, it covers the scalene muscles, levator scapulae and splenius capitis creating the fascial carpeting of the posterior triangle. The roots of cervical spinal nerves that create the cervical and brachial plexuses are located deep to it. As the trunks of brachial plexus and subclavian artery issue between the scalenus anterior and scalenus medius and move to the axilla, they carry with them a tubular sheath of the fascia, referred to as axillary sheath, which might go up to the elbow. The subclavian and axillary veins are located outside the sheath to enable their free dilation during increased venous return from the upper limb. Vertical tracing: Tracked above, the fascia goes up to the base of the skull to which it’s connected. Delineated below, it continues downwards in front of longus colli muscles into the superior mediastinum where it combines with all the anterior longitudinal ligament of the upper thoracic vertebrae (T1 to T3).
Other Features
Anteriorly, the prevertebral layer of deep cervical fascia is divided from posterior aspect of the pharynx and its covering, buccopharyngeal fascia, by a potential space referred to as retropharyngeal space. This space enables the growth of the pharynx during swallowing. The retropharyngeal space is constant with the parapharyngeal spaces at the sides of the pharynx. The retropharyngeal space is split into 2 lateral compartments (spaces of Gillette) by a midline fibrous raphe. Every lateral space includes retropharyngeal lymph nodes, which generally vanish at 3-4 years old. 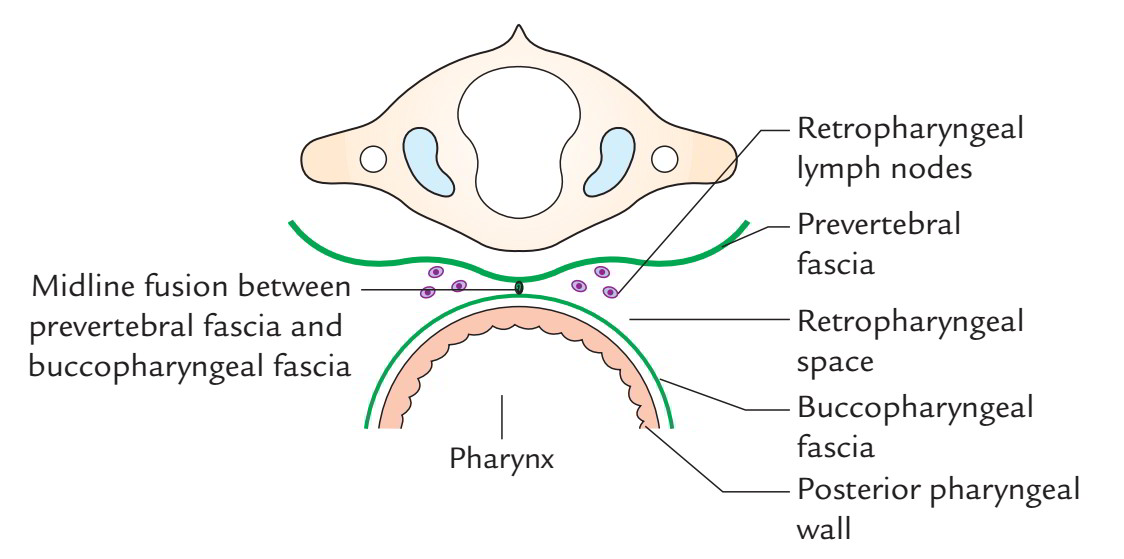 The space behind the prevertebral fascia and in front of the vertebral bodies is known as prevertebral space.
The space behind the prevertebral fascia and in front of the vertebral bodies is known as prevertebral space.
Clinical Significance
The diseases of retropharyngeal space can pass down behind the esophagus and could extend into the posterior mediastinum, of course, via superior mediastinum. The retropharyngeal abscess because of participation of retropharyngeal lymph nodes generates paramedian unilateral bulge in the posterior pharyngeal wall because of fusion of buccopharyngeal fascia to the prevertebral fascia in the median plane. Tubercular caries of cervical vertebra generate abscess in the prevertebral space which frequently extends into the retropharyngeal space. Pus accumulated in the prevertebral space on account of caries of cervical vertebrae may go forwards and cause midline bulge in the posterior pharyngeal wall. Pus may go laterally first into the posterior triangle deep to fascial carpeting created by prevertebral fascia and after that along the axillary sheath into the axilla or even into the arm.
Other Derivatives of the Deep Cervical Fascia
These contain:
- Carotid sheath.
- Buccopharyngeal fascia.
Carotid Sheath
It’s a tubular conholesation of deep cervical fascia around the (a) common carotid and internal carotid arteries and (b) internal jugular vein and vagus nerve. The vagus nerve is located posteriorly between the vein and arteries. The carotid sheath is wedged between the 3 layers of the deep cervical fascia, i.e., investing layer, pretracheal fascia and prevertebral fascia and connected to all these layers by free areolar tissue. The sheath is thick around common and internal carotid arteries but thin over the internal jugular vein to be able to enable its growth during increased venous return. 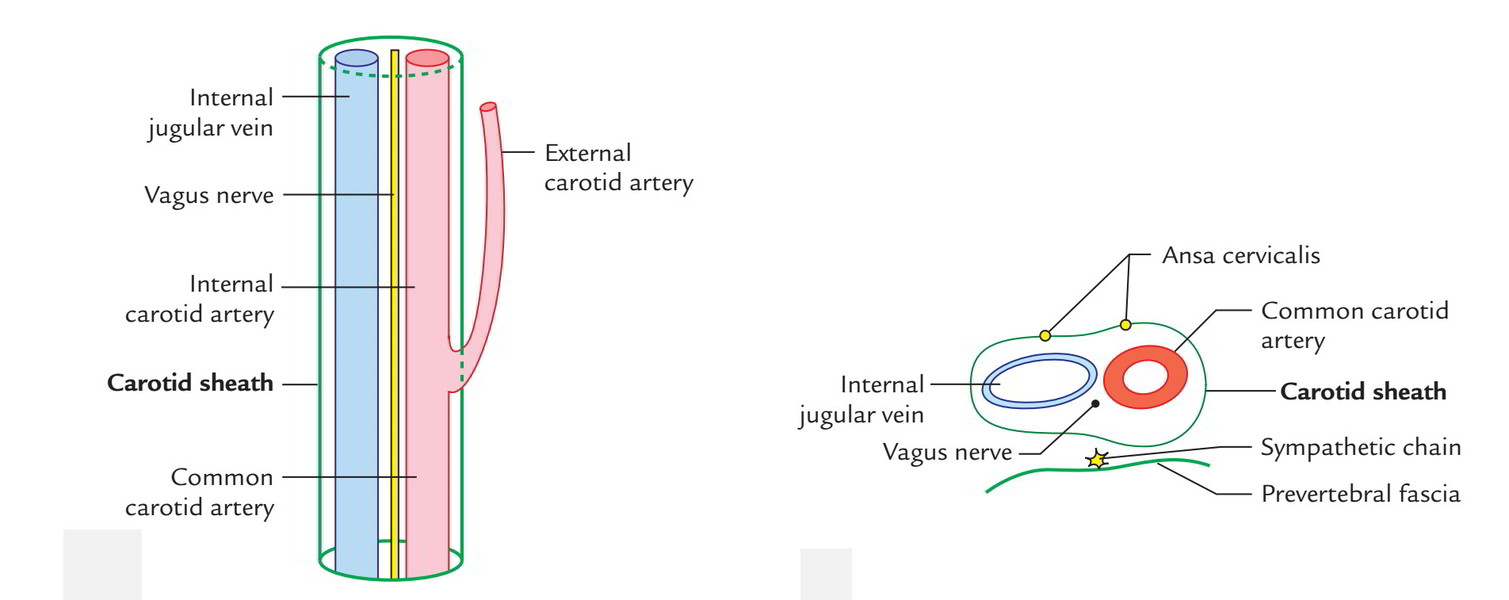 Carotid sheath goes from the base of the skull above to the arch of aorta below. At the base of the skull, it’s connected to the margins of the carotid canal and jugular fossa. At the arch of aorta, it combines with its tunica adventitia.
Carotid sheath goes from the base of the skull above to the arch of aorta below. At the base of the skull, it’s connected to the margins of the carotid canal and jugular fossa. At the arch of aorta, it combines with its tunica adventitia.
Connections
The ansa cervicalis is embedded in the anterior wall of the carotid sheath. The cervical sympathetic chain is closely linked to posterior wall of the sheath, plastered to the prevertebral fascia.
Clinical Significance
The malignant and tuberculous deep cervical lymph nodes often become adherent to the internal jugular vein. For that reason, during block dissection of the neck, the sheath is exposed and a portion of the vessel is resected to ease removal of these lymph nodes.
Buccopharyngeal Fascia
It’s a delicate and distensible layer of fascia that covers the constrictor muscles of pharynx and buccinator muscle. The buccopharyngeal fascia stretches from the base of the skull to the esophagus. Along with quite similar layer of fascia on the internal surfaces of the constrictor muscles, the pharyngobasilar fascia shuts the gaps in the muscular wall of the pharynx.

 (67 votes, average: 4.60 out of 5)
(67 votes, average: 4.60 out of 5)