The temporomandibular joint (TMJ) is a joint between temporal bone and mandible that enables the movements of the mandible for language and mastication. There are two joints, one on every side of the head,
The mandible is one bone having 2 heads, which joint on every side with temporal bone of cranium. The cranium, with which the mandible articulates, is also, mechanically one component. The movement can not take place at 1 joint if there is no co-participant movement at other joint. The temporomandibular joints are the two elements of a single craniomandibular articulation/joint. The temporomandibular joints are frequently involved in different disease processes. Thus medical students, especially dental students require to understand the anatomy of TMJ, consisting of movements and disorders connected with the joint.
Type: It’s a synovial joint of condylar variety.
Articular Surface
The upper articular surface is composed by the (a) articular fossa and (b) articular eminence of the temporal bone. This surface is concavo-convex from behind forwards.
The lower articular surface is composed by the head (condyle) of the mandible. This surface is elliptical in shape.
The articular surfaces are covered by fibrocartilage and not by hyaline cartilage, therefore temporomandibular joint is an atypical synovial joint.
Joint Cavity
The cavity of temporomandibular joint is split into upper menisco-temporal and lower menisco-mandibular compartments by an intra-articular disc of fibrocartilage.
The upper compartment allows gliding movements, on the other hand lower compartment allows gliding along with rotational movements.
Articular Disc
The articular disc is an oval plate of fibrocartilage. Though referred to as fibrocartilage, it consists primarily of collagen fibres with few cartilage cells. It’s congruent with both the articular surfaces. So its upper surface is concavo-convex (from before backwards) and its inferior surface is concave. The concavo-convex superior surface fits against the articular eminence and the concavity of the articular fossa. The lower concave surface fits with convex head of the mandible.
The periphery of the disk is connected securely to the fibrous capsule.
The disk has a thick margin, the peripheral annulus and a central depression on its inferior surface. In sagittal section, the disk seems to possess a thin intermediate zone and thickened anterior and posterior bands. The anterior group goes anteriorly via the capsule to be constant with the tendon of lateral pterygoid. The posterior band divides into 2 laminae: upper and lower. The upper lamina composed of fibroelastic tissue is connected to the squamotympanic fissure. The lower lamina composed of fibrous non-elastic tissue is connected to the rear of the condyle. The bilaminar region includes a venous plexus. The central part of the disk is avascular.
The elastic fibres in the posterior part of the disk bring back the disk in the articular fossa when the open mouth is closed.
Parts of articular disc:
In sagittal section, the articular disc of TMJ presents 5 distinct parts, from before backwards these are:
(a) anterior extension, (b) anterior thick group, (c) intermediate zone, (d) posterior thick band and (e) posterior bilaminar zone.
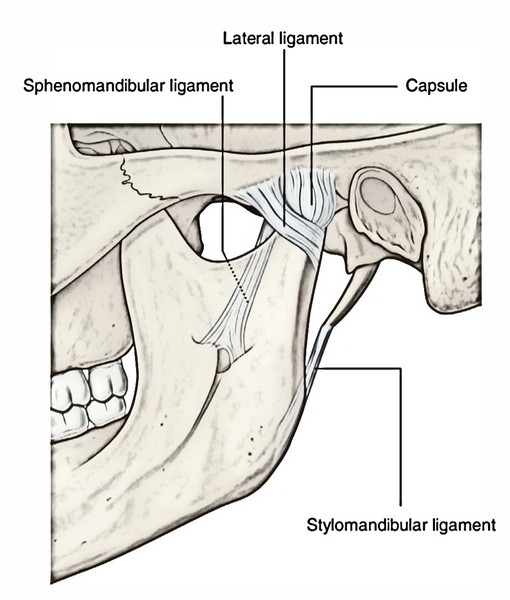
Ligaments
The ligaments are the fibrous capsule, temporomandibular, sphenomandibular and stylomandibular ligaments. The latter 2 are accessory ligaments.
Fibrous Capsule
It’s a fibrous sac to enclose the joint cavity. It’s connected above to the articular tubercle, the circumference of articular fossa and the squamotympanic fissure; and below to the neck of mandible.
The capsule is loose above the intra-articular disc and tight below it.
The synovial membrane lines the inner aspect of the fibrous capsule and the neck of the mandible.
Lateral (Temporomandibular) Ligament
It’s a true ligament and created as an outcome of thickening on the lateral aspect of the capsular ligament. Its fibres are pointed downwards and backwards. It’s connected above to the articular tubercle on the root of zygoma and below to the posterolateral aspect of the neck of the mandible. The lateral ligament reinforces the lateral aspect of the capsule.
Sphenomandibular Ligament
It’s connected above to the spine of the sphenoid and below to the lingula and lower margin of the mandibular foramen of the mandible. It is located on a deeper plane far from the joint capsule. The sphenomandibular ligament represents the unossified intermediate part of the sheath of the Meckel’s cartilage of the very first pharyngeal arch. It becomes accentuated and tight when the mandible is protruded.
Connections of Sphenomandibular Ligament
Laterally, it’s related to: (a) lateral pterygoid muscle, (b) auriculo-temporal nerve, (c) maxillary artery and (d) inferior alveolar nerve and vessels.
Medially, it’s related to: (a) medial pterygoid, (b) chorda tympani nerve and (c) wall of the pharynx.
Near its lower end the sphenomandibular ligament is pierced by mylohyoid nerve and vessels.
Clinical Significance
The sphenomandibular ligament is a significant landmark for administration of local anesthetic during inferior alveolar nerve block.
Stylomandibular Ligament
It’s connected above to the lateral surface of the styloid process and below to the angle and adjoining posterior border of the ramus of the mandible.
The stylomandibular ligament is composed because of thickening of the investing layer of deep cervical fascia, which divides the parotid and submandibular glands.
This ligament also becomes tight when the mandible is protruded.
The accessory ligaments of temporomandibular joints management range of motion (ROM) of TMJs and with mandible create a ‘swing’.
Relationships
Lateral:
- Skin and fasciae.
- Parotid gland
- Temporal branches of the facial nerve.
Medial:
- Tympanic plate dividing it from internal carotid artery.
- Spine of sphenoid.
- Auriculotemporal nerve.
- Middle meningeal artery.
- Sphenomandibular ligament.
- Chorda tympani nerve.
Anterior:
- Tendon of lateral pterygoid.
- Masseteric nerve and boats.
Posterior:
- Postglenoid part of parotid gland splitting it from external auditory meatus.
- Superficial temporal vessels.
- Auriculotemporal nerve.
Nerve Supply
Auriculotemporal nerve: Its articular twigs goes into the joint from its posterior aspect.
Masseteric nerve: Its articular twigs goes into the joint from its anterior aspect.
Blood Supply
- Maxillary artery
- Superficial temporal artery
The articular twigs of these arteries goes into the posterior aspect of the capsule.
Lymphatic Drainage
The lymph from temporomandibular joint is drained into:
- Superficial parotid (preauricular) nodes
- Deep parotid nodes
- Upper deep cervical nodes
Equilibrium
The joint is far more stable when the mouth is closed (i.e., when the teeth are in occlusion) than when the mouth is open. In occlusion, the teeth themselves brace the mandible on maxilla and no strain is thrown on the joints when an upward strike is received on the mandible. Farther in the occluded position, the forward movement of condyle is deterred by the articular eminence and by the contraction of the posterior fibres of the temporalis muscle, while the backward movement of the condyle is prevented by the lateral ligament and the contraction of the lateral pterygoid muscle.
Movements of the Mandible
When the TMJ of 2 sides are in position of remainder a small free space exists between the upper and lower teeth but lips are in contact. The different movements of mandible happen in this position.
The lower jaw can be depressed, elevated, protruded retracted and moved from side to side, by movements at temporomandibular joints.
Mechanism
All of the above mentioned movements of lower jaw entail 2 basic movements, which take place at TMJ, of course together with the aid of muscles:
- Gliding movement.
- Rotational movement.
The upper menisco-temporal compartment of TMJ allows gliding movements, during protraction (protrusion), retraction and mastication.
The lower menisco-temporal compartment allows rotation around 2 axes (a) a transverse axis, during depression and elevation and (b) a vertical axis during side to side/ chewing movements.
With these 2 types of movements, gliding and rotation and with left and right TMJs working collectively, majority of the movements of the lower jaw can be achieved absolutely as wanted. These contain opening and closing the jaws and transferring the lower jaw to side.
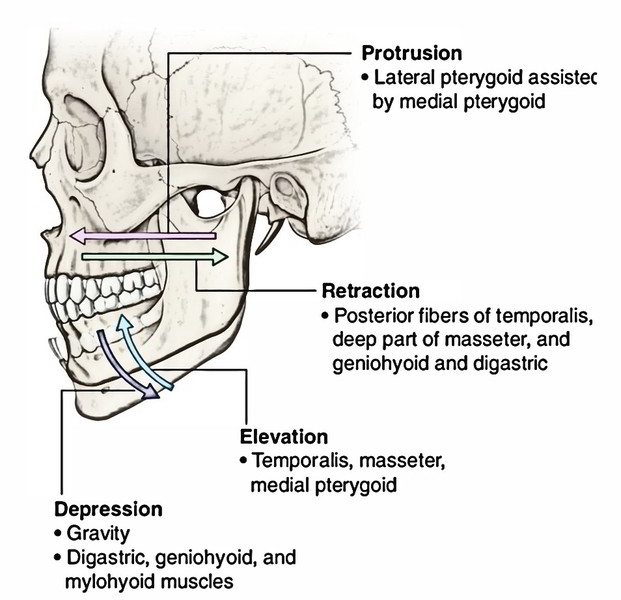
The movements happening at the temporomandibular joints are:
- Depression.
- Elevation.
- Protraction.
- Retraction.
- Side to side (Chewing) movements.
Depression (Lowering of Jaw to Open Mouth)
During depression, the head of mandible alongside an articular disc glide forwards in the upper meniscotemporal compartment on both the sides by the contraction of lateral pterygoid muscle. At exactly the same time head rotates forwards underneath the articular disc by the contraction of suprahyoid muscles, viz. digastric geniohyoid and mylohyoid. The gravity also helps in opening the mouth.
Elevation (elevating of jaw to shut the mouth): During elevation the movements take place in a reverse sequence to that of depression, i.e., first the head of mandible together with an articular disc glide backwards in the upper meniscotemporal compartment by temporalis, masseter and medial pterygoid and after that head rotates backwards on the lower surface of the disk by posterior fibres of temporalis.
Protrusion/Protraction:
In this movement, mandibular teeth move forward in front of maxillary teeth. In this act, head of mandible alongside articular disc glide forwards in the upper meniscotemporal compartment on either side by simultaneous actions of medial and lateral pterygoids of both sides.
Retraction
In this movement, the head of mandible together with articular disc glide backwards in the upper meniscotemporal compartment by the contraction of the posterior fibres of temporalis muscle and bring the joint in the resting position. The strong retraction is helped by deep fibres of masseter, digastric and geniohyoid muscles. At the conclusion of the movement the head of the mandible comes to is located underneath the articular tubercle.
Side To Side (Chewing) Movements
These movements happen alternately in the left and right temporomandibular joints. In chewing movements, the head of the mandible on 1 side glides forwards alongside the disk (as in protraction), but the head of the mandible on the opposite side just rotates on the vertical axis. As a consequence, the chin moves forwards and to 1 side, i.e., in the direction of the side on which no gliding has taken place.
In this movement, the medial and lateral pterygoids of 1 side contract instead with those of opposite sides.
The alternate movements of the sort on the 2 sides result in side to side movements of the lower jaw.
Muscles Generating Movements
Depression (Opening of Mouth)
It’s generated primarily by lateral pterygoid helped by gravity. The digastric, geniohyoid and mylohyoid muscles help when the mouth is opened extensively or against resistance.
Elevation (Shutting the Mouth)
It’s caused by medial pterygoid, masseter and temporalis (vertical fibres).
Shutting the mouth is more powerful activity in relation to the opening the mouth. As a result, when assaulted by a road dog, it’s advisable to maintain the mouth of dog closed, if possible.
Protraction
It’s done by medial and lateral pterygoids and masseter.
Retraction
It’s done by posterior fibres of temporalis. It might be helped by middle and deep fibres of the masseter, the digastric and geniohyoid muscles.
Side To Side (Mastication) Movements
These movements are performed by alternative contraction of medial and lateral pterygoids on every side.
Movements of the Mandible and Muscles Creating Them- Overview
| Movement | Muscle |
|---|---|
| Depression | Lateral pterygoid Digastric Geniohyoid Mylohyoid Gravity |
| Elevation | Masseter Medial pterygoid Temporalis |
| Protrusion | Medial pterygoid |
| (Protraction) | Lateral pterygoid |
| Retraction | Posterior fibres of temporalis |
| Side-to-side (chewing) movement | Medial and lateral pterygoids of one sidencontracting alternatively with that of opposite side |
Clinical Significance
Palpation of the Temporomandibular Joint and Related Muscles
The bilateral palpation is must to evaluate the whole joint and its related muscles. First, the patient is requested to open and shut the mouth many times. Afterward he’s requested to move the opened jaw to left and to right and eventually he’s requested to move the jaw forward. For digital palpation of condyle of moving mandible put a finger into the outer portion of the external auditory meatus.
Dislocation of the Mandible
The mandible is dislocated only anteriorly. When the mouth is open, the mandibular condyles move forward and are located underneath the articular eminences. This is the most unstable position of the temporomandibular joint. In this position, if there’s excessive opening of mouth as during yawning, unexpected violence or convulsive spasm of lateral pterygoid muscles, the head of mandible of 1 or both sides may dislocate anteriorly and get locked into the infratemporal fossa; as an effect the mouth can’t be closed anymore and any passive attempt to do that will always fracture the neck of the mandible on 1 or both sides.
To lessen dislocation, the condyle must be lowered and pushed back supporting the peak of articular eminence into the articular fossa. Consequently the decrease is done by depress-ing the jaw with thumb set on the final molar teeth and simultaneously elevating the chin.
Temporomandibular Joint Syndrome
This syndrome includes group of symptoms appearing from temporomandibular joints and their affiliated masticatory muscles. The normal presenting symptoms are:
- Diffuse facial pain, because of spasm of masseter muscle.
- Head Ache, because of spasm of temporalis muscle.
- Jaw pain, because of spasm of lateral pterygoid.
These symptoms may be connected with snapping and pain in the joint. The snapping is usually perceptible when the patient is chewing. It takes place when the posterior connection of the disk becomes stretched or detached, allowing the disk to eventually become temporarily or forever immobilized anteriorly. The derangement of articular disc results from a blockage or malocclusion.
During surgery of temporomandibular joints, the facial nerve ought to be maintained with extreme caution.
Muscles of Mastication
The muscles of mastication are concerned with movements of mandible in the temporomandibular joints during mastication.
They can be split into 2 groups:
Main muscles
- Temporalis.
- Masseter.
- Lateral pterygoid.
- Medial pterygoid.
Accessory muscles
- Digastric.
- Buccinator.
- Mylohyoid.
- Geniohyoid.
Test Your Knowledge
Temporomandibular Joint

 (63 votes, average: 4.60 out of 5)
(63 votes, average: 4.60 out of 5)