The face possesses eyes, nose and mouth. It extends superiorly up to the hair line, inferiorly up to the chin and base of the mandible and on every side up to the auricle and is the front aspect of the head. The face and the scalp have the brow in common.
Skin of the Face

Face Anatomy: Skin
The face has thick, elastic and incredibly vascular skin. The skin of the face has large number of sweat and sebaceous glands. The sebaceous glands keep the face greasy by their secretion and sweat glands help modulate the body temperature. With the exception of on the nose where it’s securely connected to the inherent cartilages and gives insertion to the muscles of facial expression, the skin of face is lax.
Clinical Significance of the Skin of the Face
Since the blood supply to the skin of the face is profuse, for that reason it’s uncommon in plastic surgery for skin flaps to necrose in this region. The laxity of greater part of skin eases fast spread of edema in the region of the face. Face is also the common site for acne as a result of presence of large number of sebaceous glands in this region.
Cleavage Lines of Skin in the Face

Face Anatomy: Cleavage Lines of Skin
The path of cleavage lines in the face changes regionally. Yet, these lines often (but not consistently) coincide with natural wrinkle lines of the face. The natural wrinkle lines result from continued folding of the skin perpendicular to the long axis of the inherent contracting muscles of facial expression. They get notable in the elderly as a result of decline of youthful skin elasticity. When the lesion of skin, viz. scars, pigmented patches, skin cancers are excised. It’s essential to give incisions along the long axis of natural wrinkle lines and the lesion ought to be enclosed in an ellipse, if the resultant scar will be aesthetically satisfactory.
Superficial Fascia of the Face
It includes muscles of facial expression, vessels and nerves and varying amount of fat. The fat is absent in the eyelids but is well grown in cheeks creating buccal pad of fat, which gives rounded contour to cheeks. The buccal pads of fat are extremely notable in infants in whom they help in suckling the milk and are named suctorial pad of fat.
Deep Fascia of the Face
The deep fascia is absent in the region of face with the exception of over the parotid gland and masseter muscle that are covered by parotidomasseteric fascia. The absence of deep fascia in the face is crucial for the facial expression.
Muscles of Facial Expressions

Face Anatomy: Muscles of Facial Expressions
The muscles of facial expression are embedded in the superficial fascia of the face. The majority of them originate from bones of the skull and are added into the skin. They bring about various types of facial expressions, thus the name muscles of facial expression, the activities of many are indicated by their names.
Characteristic Features of the Muscles of Facial Expression
The features of the muscles of facial expressions are as follows:
- They is located in superficial fascia and fit into the skin.
- Morphologically, they represent the specialized members of the subcutaneous muscle (panniculus carnosus), of lower creatures.
- Embryologically, they grow from mesoderm of second pharyngeal arch, therefore supplied by facial nerve, the nerve of second arch.
- Functionally, they perform all significant functions of non-verbal communication along with shutting and opening the orifices in the region of the face.
Location and Function
The facial muscles are arranged in groups around the orifices of mouth, eye and nose as sphincters and dilators of these orifices. Along with modulating the opening and closure of these orifices, as mentioned before, they create distinct types of facial expressions. To perform fine movements of facial expressions the facial muscles have small motor units. Though all these muscles are essential for facial expression, the pupils are counseled not to load their recollection by making use of their attachments. Nevertheless, they ought to understand the significance of orbicularis oculi, orbicularis oris and buccinator for the serious effects following their paralysis. Along with muscles around the eye, nose and mouth, the muscles of facial expression also contain the muscles of scalp, auricle and the subcutaneous muscle of the neck- the platysma.
Muscles Around the Orifice of the Eye
These contain:
- Orbicularis oculi.
- Corrugator supercilii.
- Frontalis.
- Levator palpebrae superioris.
Orbicularis oculi
It includes 3 parts:
- Orbital part: It originates from medial palpebral ligament, frontal process of maxilla and adjoining part of the frontal bone. The fibres create entire elliptical loops on and around the orbital margin, without gap before returning to their point of origin. It shuts the eye closely to guard the eye from extreme light and dust particles. It’s also utilized by men and women for winking.
- Palpebral part: It originates from medial palpebral ligament and sails laterally over the upper and lower eyelids to be added into the lateral palpebral ligament. A small group of fibres referred to as ciliary bundle is located along the margins of both eyelids. It closes the eyelids softly as in sleep or in blinking.
- Lacrimal part: It is located behind the lacrimal sac. It originates from posterior lacrimal crest and lacrimal fascia creating a sheath of lacrimal sac that enters laterally in front of tarsal plates of both eyelids to be fit into the lateral palpebral raphe. It dilates the lacrimal sac by using traction on the lacrimal fascia, thereby helping in the drainage of lacrimal fluid.
Clinical significance
Crow’s feet: The contraction of whole orbicularis oculi pulls the skin of forehead, temple and cheek in the direction of the lateral angle of the eye, creating radiating skin folds from the lateral angle of the eye, which might be a permanent feature in a few old folks creating the so called crow’s feet.
Ectropion
The paralysis of orbicularis oculi ends in drooping of the lower eyelid (ectropion) causing spilling of tear on the cheek (epiphora).
Corrugator Supercilii
It originates from the medial end of the superciliary arch, enters laterally and upwards to be added into the skin of the eyebrow above the middle of the supraorbital margin. It hauls the eyebrow medially and downwards creating vertical wrinkles on the brow as in frowning, an expression of irritation.
Frontalis
It’s already explained in the section on scalp. The frontalis elevates the eyebrows and creates transverse wrinkles on the brow as an expression of surprise, dread or fright.
Levator Palpebra Superioris
It’s not a muscle of the face however among the orbital muscles, thus described in detail under orbit. Levator palpebrae superioris is an antagonist to the sphincteric activity of palpebral part of orbicularis oculi. It elevates the upper eyelid.
Muscles around the Nasal Cavity
The muscles connected with nasal cavity are as follows:
- Procerus.
- Nasalis.
- Depressor septi
These muscles are poorly grown because anterior nares are open.
Procerus
It appears from nasal bone, enters upwards to be added into the skin of the lower part of the brow. It creates transverse wrinkles around the bridge (root) of the nose as in frowning.
Nasalis
It contains 2 parts: transverse part termed compressor naris and alar part named dilator naris. Compressor naris appears create maxilla near the nasal notch, enters upwards and medially to create an aponeurosis on the other side of the bridge of nose where it becomes constant with its counterpart on the opposite side. It compresses the nasal aperture. Dilator naris appears from maxilla from the margin of the nasal notch and fit into the lateral part of the ala of the nose. It dilates the anterior nasal apertures as in deep inspira-tion. It also expresses the fury (hint of omega).
Depressor septi
It appears from the incisive fossa of the maxilla and is added into the lower mobile part of the nasal septum. It fixes the nasal septum to enable dilatation of anterior nasal aperture by dilator naris.
Muscles around the Mouth
The muscles around the mouth are liable for the movement of lips and cheek. These contain:
- Orbicularis oris: Actions as sphincter.
- 9 muscles converging around the mouth serve as dilators.
Orbicularis Oris

Face Anatomy: Orbicularis Oris
This complex muscle encompasses the oral orifice and creates the greater part of the lips. It’s extrinsic and intrinsic portions. The major extrinsic (or superficial) portion consists of interlacing fibres of the muscles which converge around the mouth for their insertion into the lips, viz. levator anguli oris, depressor anguli oris, buccinator, etc. Majority of the fibres come from buccinator. The fibres of buccinator converge in the direction of the modiolus. At modiolus they create chiasma. The uppermost and lowermost fibres pass straight in their various lips, while the middle fibres decussate, so the upper fibres enter the lower lip and lower into the upper lip. The intrinsic portion is composed of fibres running obliquely between the skin and mucus membrane of the lips and incisive pas, which pass laterally into the lips from the jaws adjacent to the incisor teeth and interlace with the fibres ofperipheral part of orbicularis oris as they method the modiolus.
Nerve Supply: Buccal branch of the facial nerve.
Activities: Due to its complex nature, orbicularis oris is effective at creating wide selection of movements of lips like shutting, pouting, pursing, twisting, etc.
Clinical significance
Paralysis of orbicularis oris: The paralysis of 1-half of orbicularis oris prevents the correct close of lips on this side. Thus the address is slurred and the spit escapes between the lips at the angle of the mouth (dribbling of spit from the angle of the mouth).
9 Muscles Converging Around the Mouth
All these are as follows:
- Levator labii superioris alaeque nasi.
- Levator labii superioris.
- Levator anguli oris.
- Zygomaticus minor.
- Zygomaticus major.
- Depressor labii inferioris.
- Depressor anguli oris.
- Risorius.
- Buccinator.
The muscle of chin named mentalis is normally discussed with muscles around the mouth.
- Levator labii superioris alaeque nasi originates from the frontal process of the maxilla and is added in the ala of nose by 1 slip and to the upper lip by another skid. It elevates the upper lip and helps to dilate the nostril.
- Levator labii superioris originates from maxilla just above the infraorbital foramen and is added into the upper lip. It elevates the upper lip.
- Levator anguli oris originates from maxilla below the infraorbital foramen and is added into the angle of the mouth. It is located deep to levator labii superioris. It lifts the angle of the mouth.
- Zygomaticus minor originates from zygomatic bone and is inserted into the upper lip. It elevates the upper lip.
- Zygomaticus major originates from zygomatic bone and is added into the angle of the mouth. It pulls the angle of the mouth upward and laterally.
- Depressor labii inferioris originates from the anterior oblique line of the mandible and is added into the lower lip. It pulls the lower lip downwards and somewhat laterally.
- Depressor anguli oris originates from the posterior part of the oblique line of the mandible and is fit into the angle of the mouth. It pulls the angle of the mouth downwards and laterally.
- Risorius originates from parotid fascia as a continuance of posterior fibres of platysma and is fit into the angle of the mouth. It retracts the angle of the mouth softly.
- Mentalis, a small conical muscle originates from the incisive fossa of the mandible and is added into the skin of the lower lip. It puckers the chin and protrudes the lower lip.
- Buccinator (Bugler’s muscle/trumpeter’s muscle) is muscle of the cheek and demands.

Face Anatomy: Converging Muscles around the Mouth
After origin, the fibres run in the direction of the mouth and fill the gap between the upper and lower jaws. The fibres are ordered into upper, intermediate and lower groups. Insertion: The buccinator is added in a complex way into the upper and lower lips. When it reaches near the angle of the mouth:
- Upper fibres enter upper lip,
- Lower fibres enter the lower lip and
- Intermediate fibres decussate and as a result upper fibres of the group enter lower lip and lower fibres enter the upper lip.
Nerve Supply: Buccal branches of facial nerve. Activities: It flattens the cheek against the gum and teeth and thereby prevents the accumulation of food in the vestibule of mouth during mastication. It’s responsible for blowing the cheek and expelling the air between the lips from inflated vestibule as in blowing the trumpet (therefore the name trumpeter’s muscle). The outer surface of buccinator muscle is covered by buccopharyngeal fascia and its inner surface is lined by a mucus membrane. It’s pierced by parotid duct. The pterygomandibular raphe divides it from superior constrictor of the pharynx. A gap between maxillary fibres and those from pterygomaxillary raphe gives passage to the tendon of tensor palati.
Clinical significance
Paralysis of buccinator muscle: If the buccinator muscle is paralyzed, as it happens in facial palsy, the food collects in the vestibule of mouth during mastication and the man can not blow his cheek. Modiolus: It’s a holese, compact, mobile, fibromuscular mass situated about 1.25 cm lateral to the angle of the mouth. It’s created because of interlacing of fibres of 5 muscles which converge in the direction of the angle of the mouth. These muscles (modiolar muscles) are: levator anguli oris, zygomaticus major, buccinator, depressor anguli oris and risorius. 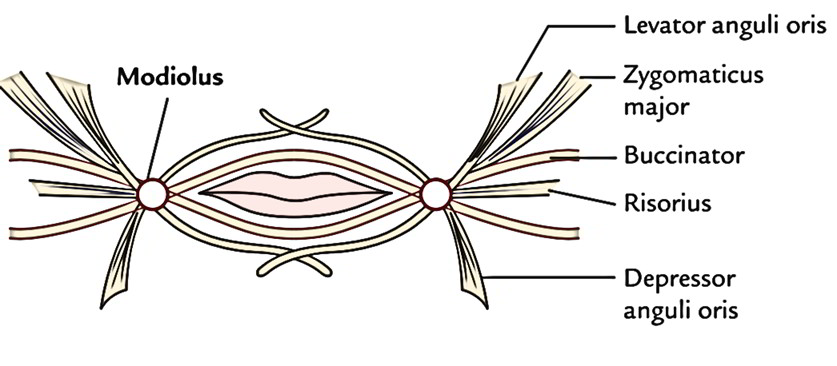 It can be easily felt by using opposed thumb and index finger to compress the skin and mucosa simultaneously. The pulsations of facial artery can be felt just lateral to the modiolus. The inadvertent damage of modiolus during plastic surgery contributes to unacceptable facial asymmetry.
It can be easily felt by using opposed thumb and index finger to compress the skin and mucosa simultaneously. The pulsations of facial artery can be felt just lateral to the modiolus. The inadvertent damage of modiolus during plastic surgery contributes to unacceptable facial asymmetry.
Facial Muscles and Emotional Expressions
Facial muscles and emotional expressions.
| Emotional expression | Presenting features | Facial muscle/muscles |
|---|---|---|
| Surprise/horror/fright | Transverse wrinkles of the forehead | Frontalis |
| Frowning | Vertical wrinkles of the forehead. Transverse wrinkle across the root of nose | Corrugator supercilii. Procerus |
| Anger | Dilation of the anterior nasal aperture. Depression of lower mobile part of the nasal septum | Dilator naris Depressor septi |
| Laughing | Angle of mouth drawn upwards and laterally | Zygomaticus major |
| Sadness/sorrow/grief | Accentuation of nasolabial fold. Elevation and eversion of the upper lip. | Levator labii superioris. Levator anguli oris and zygomaticus minor. |
| Angle of mouth drawn downwards and laterally | Depressor anguli oris | |
| Grinning | Retraction of angle of the mouth laterally | Risorius |
| Disdain/doubt | Puckering of the chin, protrusion of lower lip | Mentalis |
| Worry | Skin folds radiating laterally from lateral angle of the eye | Orbicularis oculi |
| Irony | Angle of the mouth drawn downwards and somewhat laterally | Depressor labii inferioris |
Clinical Testing of The Muscles of Facial Expression
The muscles of facial expression are called for in facial nervelesion. They can be analyzed medically in these manners:
- Frontalis, by requesting the patient to look upwards without moving his head and after that look for horizontal wrinkles on the brow.
- Corrugator supercilii, by requesting the patient to frown and after that look for vertical wrinkles between both eyebrows.
- Orbicularis oculi, by requesting the patient to shut the eyes closely.
- Orbicularis oris, by requesting the patient to whistle.
- Dilators of the mouth, by requesting the patient to reveal his teeth.
- Buccinator, by requesting the patient to smoke his mouth and after that blow out the air powerfully.
- Zygomaticus major, by requesting the patient to laugh.
- Risorius, by requesting the patient to smile softly.
Nerve Supply
Motor Nerve Supply

Face Anatomy: Motor Nerve Supply
The motor Nerve Supply of the face is originated from the facial nerve. After coming out of cranial cavity via stylomastoid foramen, the facial nerve wind around the lateral aspect of styloid process and after that enters the parotid gland Here it breaks up into 5 terminal branches (viz. temporal, zygomatic, buccal, marginal mandibular and cervical), which come forth in the face radiating via the anterior border of the parotid gland and supply the muscles of facial expression. These 5 sets of terminal branches create the goosefoot pattern (pes anserinus) on the face. Innervation of muscles of facial expression by the terminal branches of facial nerve.
| Terminal branches of facial nerve | Muscles innervated |
|---|---|
| Temporal branch | Upper part of the orbicularis oculi. Frontalis. Corrugator supercilii |
| Zygomatic branch | Lower part of the orbicularis oculi |
| Buccal branches | Zygomaticus major and minor |
| a). Upper buccal branch | Levator anguli oris. Levator labii superioris. Levator labii superioris alaeque nasi. Muscles of the nose |
| b). Lower buccal branch | Buccinator. Orbicularis oris |
| Marginal mandibular branch | Risorius. Depressor anguli oris. Depressor labii inferioris4Mentalis |
| Cervical branch | Platysma |
Clinical Significance
Bell’s palsy: It’s lower motor neuron type paralysis of facial muscles because of compaction of facial nerve in the facial canal near stylomastoid foramen. The precise etiology isn’t understood but it’s likely because of viral infection. Features on the Side of Paralysis.
- Facial asymmetry (affected side is pulled to the healthy side) – because of unopposed activity of muscles of normal side.
- Loss of horizontal wrinkles on brow- because of paralysis of occipitofrontalis muscle.
- Widening of palpebral fissure and inability to shut the eye- because of paralysis of orbicularis oculi.
- Tears flow down from the eye (epiphora) because of paralysis of the lower part of the orbicularis oculi.
- Sagging of the angle of the mouth in the direction of the affected side and inability of the angle of the mouth to move upwards and laterally during laughing- because of paralysis of zygomaticus major.
- Loss of nasolabial furrow- because of paralysis of levator labii superioris alaeque nasi.
- Accumulation of food into the vestibule of the mouth- because of paralysis of buccinator muscle.
- Dribbling of spittle from the angle of the mouth- because of paralysis of orbicularis oris.
- Loss of resistance when one presses cheek with inflated vestibule and air leaks out from between the lips- because of paralysis of buccinator muscle.

Face Anatomy: Face deformation

Face Anatomy: Cutaneous Nerves
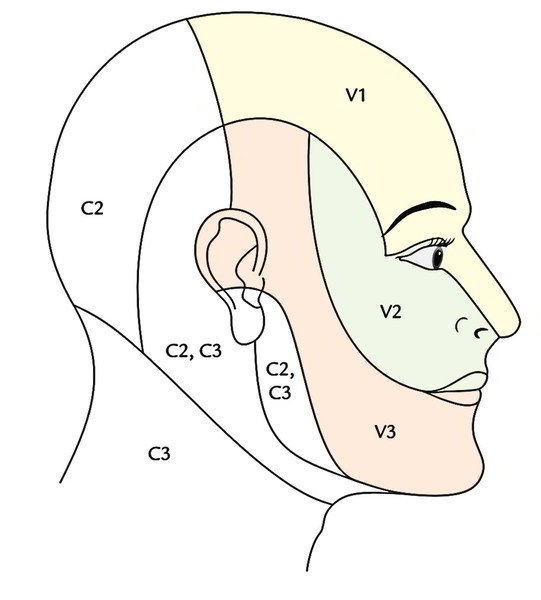
In upper motor neuron type paralysis of facial muscles because of engagement of the pyramidal tract, the upper part of the face isn’t changed. This part of face stays normal because lower motor neurons supplying this part of face get corticonuclear fibres (upper motor neurons) from cerebral cortex of the both sides. Sensory Nerve Supply The trigeminal nerve is the sensory nerve of the face for the reason that it supplies all of the face, with the exception of skin over the angle of mandible that is supplied by great auricular nerve originated from ventral rami of the second and third cervical nerves (C2, C3). The upper one-third face (developing from frontonasal process) is supplied by ophthalmic section, middle third of face (developing from maxillary processes) is supplied by maxillary section and lower third of face (developing from mandibular processes) is supplied by mandibular division of the trigeminal nerve. The territories of cutaneous innervation of ophthalmic, maxillary and mandibular nerves aren’t horizontal, but arch in the posterosuperior way, showing the direction of development of brain and head. So the first beard area was drawn up to the temple and essentially the neck skin is drawn up to overlap the angle of the mandible. This describes the innervation of face by the second cervical nerve (C2). The cutaneous nerves of the face originated from 3 sections of the trigeminal nerve are as follows: Branches of ophthalmic division of trigeminal nerve:
- Supraorbital.
- Supratrochlear.
- Infratrochlear.
- External nasal.
- Lacrimal.
Branches of maxillary division of trigeminal nerve:
- Infraorbital.
- Zygomaticofacial.
- Zygomaticotemporal.
Branches of mandibular division of trigeminal nerve:
- Mental.
- Buccal.
- Auriculo temporal
Clinical Significance
Trigeminal neuralgia (tic douloureux): It’s a clinical condition characterized by unexpected paroxysmal attacks of lancinating pain continuing from few hours to many days, confined to distribution of one or more sections of trigeminal nerve. It usually begins in the maxillary land and more often on the right side. Herpes zoster ophthalmicus: It’s a viral infection involving the ophthalmic nerve. It presents as acute pain and edema in the ophthalmic terrain and is defined by the look of vesicles along the course of cutaneous branches of the ophthalmic nerve.
Arterial Supply of the Face

Face Anatomy: Arterial Supply of the Face
The face is the highly vascular region and is supplied by these arteries:
- Facial artery.
- Transverse facial artery.
- Arteries that accompany the cutaneous nerves.
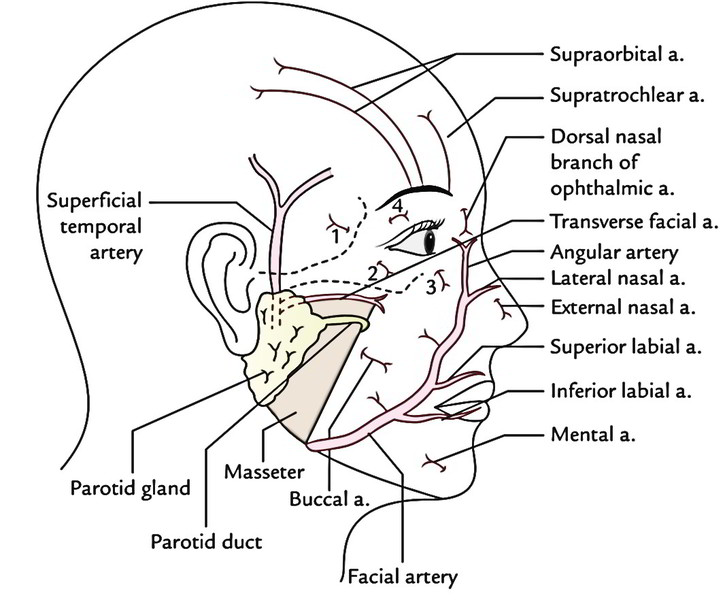 The primary arterial supply to the face is by the facial artery, thus it’s named primary artery of the face.
The primary arterial supply to the face is by the facial artery, thus it’s named primary artery of the face.
Facial Artery
It appears from external carotid artery in the neck in the level of greater cornu of the hyoid bone and following a looped course in the submandibular region, it enters the face by winding around the lower border of the mandible in the anteroinferior angle of the masseter by piercing the investing layer of deep cervical fascia. In the face, the artery enters tortuously, first upwards and forwards to a point 1.25 cm lateral to the angle of the mouth and after that ascends along the side of the nose to the medial angle of the eye where it stops by anastomosing with the dorsal nasal branch of ophthalmic artery. The terminal part of facial artery is termed angular artery.
Branches of the Facial Artery in the Face
In the face it supplies 3 sets of termed branches:
- Inferior labial artery, to supply the lower lip.
- Superior labial artery, to supply the upper lip.
- Lateral nasal artery, to supply the ala and dorsum of the nose. All these branches originate anteriorly.
- Muscular branches, are small, unnamed and originate from the posterior aspect of the artery.
Key Points The tortuosity of facial artery keeps its walls from being unduly stretched during the movements of mandible, lips and cheeks. The facial artery takes part in the formation of numerous anastomoses, viz. 1. Across the midline with the branches of the opposite side. In the lips, the anastomoses between the superior and inferior labial arteries of 2 sides are large and so efficient that if cut blood spurts from both wound ends. 2. At the medial angle of eye, it anastomoses with the branches of ophthalmic artery, a branch of internal carotid artery and thus the site of anastomosis between the branches of external and internal carotid arteries.
Clinical Significance
Since the face is amply vascular, the wounds of face bleed profusely but luckily they heal fast. The pulsations of facial artery can be felt at 2 sites, viz.
- At the base of the mandible close to anteroinferior angle of the masseter.
- About 1.25 cm lateral to the angle of the mouth.
Transverse Facial Artery
It’s a small artery that originates from superficial temporal artery, inside the parotid gland After appearing from parotid gland it runs forwards on the masseter between the zygomatic arch and the parotid duct escorted by buccal branch of the facial nerve.
Arteries Accompanying the Cutaneous Nerves
They may be small and generally go undetected but a few of them can be easily observed, viz. infraorbital artery, buccal artery and mental artery. Notice, they all are originated from maxillary artery.
Venous Drainage of the Face
The venous blood from the face is emptied by 2 veins:
- Facial vein.
- Retromandibular vein.

Face Anatomy: Venous Drainage of the Face
Facial Vein
It’s the largest vein of the face. It’s created at the medial angle of the eye by the union of supratrochlear and supraorbital veins. After formation, it runs straight downwards and backwards behind the facial artery to get to the anteroinferior angle of the masseter. Here it pierces the deep fascia, crosses superficial to submandibular gland and joins the anterior section of retromandibular vein below the angle of the mandible to create the common facial vein, which empties into the internal jugular vein. The tributaries of facial vein correspond to the branches of facial artery.
Deep Connections in the Face
The facial vein interacts with the entire cavernous sinus via the following 2 courses:
- At the point of commencement, the facial vein commu-nicates with the superior ophthalmic vein, which enters backwards inside the orbit and drains into cavernous sinus.
- In the cheek, the facial vein is joined to the pterygoid venous plexus by the deep facial vein. The deep facial vein enters backwards over the buccinator deep to the ramus of the mandible and interacts with all the pterygoid venous plexus around the lateral pterygoid muscle, which in turn communicates with the entire cavernous sinus via an emissary vein.
Clinical Significance

Face Anatomy: Dangerous Area of the Face
Dangerous area of the face: The facial vein and its communications are devoid of valves in their own lumens. Since facial vein rests directly on the muscles of facial expression, the movements of these muscles may ease the spread of septic emboli from contaminated area of the lower part of the nose, upper lip and adjoining part of the cheek in retrograde way via deep facial vein, pterygoid venous plexus and emissary vein into the cavernous sinus resulting in meningitis and cavernous sinus thrombosis. Because of this, this portion of the face is named dangerous area of the face.
Retromandibular Vein
The retromandibular vein is composed by the union of the superficial temporal and the maxillary vein inside the parotid gland. On leaving the parotid gland, it splits into 2 sections: anterior and posterior. The anterior section joins the facial vein to create the common facial vein on the other hand posterior section joins the posterior auricular vein to create the external jugular vein.
Lymphatic Drainage of the Face

Face Anatomy: Lymphatic Drainage of the Face
The face is split into 3 lymphatic lands:
- Upper land: Constituting greater part of the fore-head, afterwards halves of the eyelids consisting of conjunctiva, parotid area and adjoining part of the cheek. Lymph from upper land is drained into preauricular lymph nodes (also termed superficial parotid lymph nodes).
- Middle land: Containing central part of the fore-head, medial halves of the eyelids, external nose, upper lip, lateral part of lower lip, medial part of cheek and greater part of the lower jaw. Lymph from middle land is drained into subman-dibular lymph nodes.
- Lower land: Constituting central part of the lower lip and chin. Lymph from lower land is drained into submental lymph nodes.

 (60 votes, average: 4.30 out of 5)
(60 votes, average: 4.30 out of 5)